
Medical Image of the Week: Lemierre Syndrome
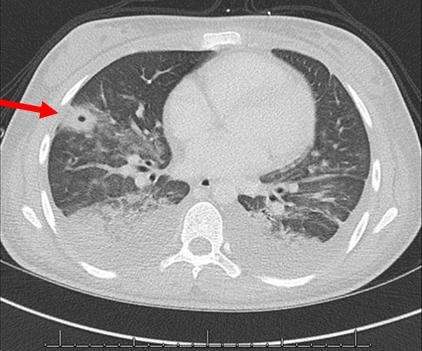
Figure 1. CT scan of chest (axial image) demonstrating peripheral cavitating lesion (arrow) with multifocal ground glass opacities and bilateral pleural effusions.

Figure 2. CT scan of neck, soft tissue (coronal [A], axial [B] image) demonstrating a partially occlusive thrombus in the left internal jugular vein (coronal red arrows, axial green arrow).
A previously healthy 18-year-old girl was evaluated at an urgent care center for a three day history of sore throat, fever, nausea, vomiting, diarrhea, and myalgias; the diagnosis of influenza was made at that time. Four days later, she presented to our Emergency Department with sore throat, left sided neck pain and swelling, productive cough, fever, worsening dyspnea, and pleuritic chest pain. On examination her temperature was 36.9 °C, heart rate was 142 beats per minute, and respiratory rate was 18 breaths per minute. She had enlarged tonsils without exudates, cervical and submandibular lymphadenopathy, and tenderness of her left lateral neck. Lung examination showed increased work of breathing with decreased breath sounds at the bases. Laboratory evaluation revealed an elevated white count (17,000 cells/µL) with 91% neutrophils, elevated blood urea nitrogen (21 mg/dL), creatinine (1.6 mg/dL), and venous lactate (4.0 mMol/L). Initial chest radiograph showed no evidence for acute cardiopulmonary process. She was admitted, blood cultures were drawn, and treatment for sepsis with vancomycin, xeftriaxone, and azithromycin was initiated. Subsequent chest radiograph demonstrated an ill-defined airspace opacification in the right lower lobe.
Computed tomographic (CT) imaging of the chest showed multifocal ground glass opacities and areas of consolidation with cavitation, consistent with septic embolic disease (Figure 1). Blood cultures grew Streptococcus anginosus and Fusobacterium necrophorum. CT imaging of the neck showed a partially occlusive thrombus in the left internal jugular vein (Figure 2). The diagnosis of Lemierre’s syndrome was made. The patient required chest tube drainage for bilateral empyema and was treated with 3 weeks of ampicillin followed by 3 weeks of high dose amoxicillin-clavulanate; she recovered completely.
Lemierre's syndrome, or anaerobic postanginal sepsis, was first described by Andre Lemierre in 1936. It is characterized by thrombophlebitis of the internal jugular vein and bacteremia caused by organisms of the normal oropharyngeal bacterial flora, classically Fusobacterium necrophorum. Lemierre’s syndrome is most commonly preceded by pharyngitis or tonsillitis, but can also be associated with odontogenic infections or otitis media. The primary infection progresses from the oropharynx and invades the lateral pharyngeal space, eventually leading to thrombophlebitis of the internal jugular vein. A majority of patients develop septic emboli, as seen in our patient, with the lungs and large joints being the most common sites of metastasis. Lemierre’s syndrome predominantly affects previously healthy children, adolescents, and young adults with most cases presenting in the second decade of life. Common physical findings include severe pharyngitis, cough/hemoptysis, dyspnea, and tenderness and swelling over the internal jugular vein. Diagnosis is confirmed by the presence of thrombophlebitis of the internal jugular vein and anaerobic organisms such as F. necrophorum in the bloodstream.
Elisa Phillips BA, BS*, Ziad Shehab MD**, and Daniela Lax MD***
*The University of Arizona College of Medicine; **Department of Pediatrics, Division of Infectious Disease; and ***Banner – University Medical Group, Pediatric Cardiology
University of Arizona
Tucson, AZ USA
References
- Bliss SJ, Flanders SA, Saint S. Clinical problem-solving. A pain in the neck. N Engl J Med. 2004 Mar 4;350(10):1037-42. [CrossRef] [PubMed]
- Kuppalli K, Livorsi D, Talati NJ, Osborn M. Lemierre's syndrome due to Fusobacterium necrophorum. Lancet Infect Dis. 2012 Oct;12(10):808-15. [CrossRef] [PubMed]
- Eilbert W, Singla N. Lemierre's syndrome. Int J Emerg Med. 2013 Oct 23;6(1):40. [CrossRef] [PubMed]
Cite as: Phillips E, Shehab Z, Lax D. Medical image of the week: Lemierre syndrome. Southwest J Pulm Crit Care. 2017;15(5):223-4. doi: https://doi.org/10.13175/swjpcc135-17 PDF
 Post a Comment
Post a Comment
Reader Comments