
Manuscript Guidelines
October 2024
Manuscripts must be submitted online to the editor at rickrobbins@cox.net (preferred) or via the SWJPCC website. Remember to include your email address especially if submitting through the website.
Mission Statement
The Southwest Journal of Pulmonary, Critical Care & Sleep publishes high-quality original papers, reviews, clinical trials and case presentations in respiratory, critical care, and sleep medicine to foster advances in translational research and clinical practice.
Aims and Scope
Format of the Manuscript
File format
Standard word processing software (Microsoft Word preferred). Figures may be inserted into the manuscript or in a separate file; see next section for instructions. Text: single-spaced, 12 point type; Arial (preferred), Times Roman or Helvetica font. Pages should be numbered consecutively beginning with the title page.
Parts of paper
- Title page
- Abstract (if applicable)
- Abbreviation list (if applicable)
- Body of paper
- Introduction
- Methods
- Results
- Discussion
- Acknowledgments
- References
- Figure legends (or in body of paper if figures are also in body)
- Tables (or in body of paper)
Title Page
Each manuscript must include a title page including the following:
- Full article title;
- Full first and last names and e-mail addresses;
- Use initials if appropriate provide highest academic degrees for all authors and institutional affiliations for all authors provide corresponding author full address and e-mail address.
The institution(s) and city, state and country where the work was performed;
Disclosure of any personal or financial support or author involvement with organization(s) with financial interest in the subject matter – or any actual or potential conflict of interest – and if no conflicts exist, a statement to that effect must be included for each author. [Note: The corresponding author is responsible for providing the current e-mail addresses for all coauthors so that they can receive notification
Abstract
Abstracts are by far the most read portion of a manuscript, so authors should take particular care in crafting this portion of the paper. See Table 1 for guidance on the need and length of abstracts.
For Original Research, provide a structured abstract not to exceed 250 words. Structured abstracts should consist of four sections, labeled as Background, Methods, Results, and Conclusions. The sections should briefly describe, respectively, the problem being addressed in the study, how the study was performed (including numbers of patients or laboratory subjects), the significant results, and what the authors conclude from the results. For all clinical trials the clinical trial registry name and registration number must be stated at the end of the Abstract as a final paragraph.
Abbreviation List
On a separate page in your manuscript, please provide an alphabetical list of all abbreviations used in the paper, followed by their full definitions. Each abbreviation should be expanded at first mention in the text and noted parenthetically after expansion. To aid readers, please use abbreviations sparingly.
Body of Paper
Subheads should be used to provide guidance for the reader; this format can be flexible, but the subheads in Original Research would ordinarily include sections such as Introduction, Methods, Results, and Discussion.
Detailed instructions on how to prepare and format articles for the following sections: Case Reports, Case Series/Reports, Imaging and Pathology for Clinicians, Correspondence and Transparency in Medicine, Medical Image of the Week and Case of the Month are below.
When mentioning products such as drugs or equipment, use the generic (nonproprietary) name, followed in parentheses by the brand or trade name, manufacturer name, and manufacturer location, as in the following example: The patient was treated with bi-level nasal positive pressure (BiPAP; Respironics Inc; Murrysville, PA).
Acknowledgments
Each Original Research paper may have an Acknowledgments section that describes the role of each author in the preparation of the manuscript. Each paper may have a section that provides information on the funding sources for the paper. Any person who contributed to the paper without qualifying for authorship should be acknowledged. If a professional medical writer or editor was used, the source of payment should be referenced. See recent issues for guidance on how to format.
References
Authors are responsible for the accuracy and completeness of citations. In text, references must be given numbers in parentheses consecutively in the order in which they appear in the text. The full citations must be listed on a separate sheet in numerical order at the end of the text. Each reference must contain, in order, the following: authors (last name, initials) [all listed if up to six; first three followed by “et al” in the case of more than six authors], title of article (lowercase, no quotation marks), source, year of publication, volume, issue, and inclusive page numbers. No spaces should be used from the year of publication through the final page number. References to abstracts or letters may be included but must be noted as such. Abbreviations of journal names must conform to Index Medicus style (available online at ftp://nlmpubs.nlm.nih.gov/online/journals/ljiweb.pdf). Please note that no periods should be used after authors’ initials or after journal abbreviations; however, periods should be inserted after the publication name and at the end of each reference. Please include the digital object identifier (doi) and the PubMed identifier (PMid) and/or PubMed Central reference number (PMCid) after each reference if known.
Following are examples of the most common formats.
Journal Article
- Sillen MJH, Speksnijder CM, Eterman R-MA et al. Effects of neuromuscular electrical stimulation of muscles of ambulation in patients with chronic heart failure: a systematic review of the English-language literature. Chest. 2009;136(1):44-61. doi: http://dx.doi.org/10.1378/chest.08-2481 PMid:19363213
- Barker E, Haverson K, Stokes CR, Birchall M, Baily M. The larynx as an immunological organ: immunological architecture in the pig as a large animal model. Clin Exp Immunol. 2006;143(1):6-14. doi: http://dx.doi.org/10.1111/j.1365-2249.2005.02950.x PMid:16367928 PMCid:PMC1809556
Book
- Shields TW, LoCicero J III, Reed CE, Feins RH. General Thoracic Surgery. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:200-232.
Book Chapter
- Stone AC, Klinger JR. The right ventricle in pulmonary hypertension. In: Hill NS, Farber HW, eds. Pulmonary Hypertension. New York, NY: Humana Press; 2008:93-126.
Abstract
- Garg N, Garg G, Christensen G, Singh A. Acute coronary syndrome caused by coronary artery mycotic aneurysm due to methicillin-resistant staphylococcus aureus [abstract]. Chest. 2008;134(suppl):1001S.
For assistance in formatting other types of references, please refer to the American Medical Association (AMA) Manual of Style.2 (p 39-80)
Figure Legends
All illustrations must be cited in consecutive numerical order within the text of the manuscript. A legend for each illustration should be provided on a separate page of the manuscript, not on the figure itself. Please identify stains and magnifications for all photomicrographs. If permission was needed for a figure, please acknowledge the source in the caption and provide the full reference in the reference list. If there is a possibility that an individual can be identified, Southwest Journal of Pulmonary & Critical Care must receive a copy of the release, and a statement that permission to use the image was granted should be in the caption.
Tables
Tables should be self-explanatory and should not duplicate textual material. They must be numbered and cited in consecutive order in the text, and each must have a succinct title, and (where appropriate) a legend describing abbreviations and footnotes at the bottom of the table. See past issues for guidance on how to format footnotes. Tables consisting of more than 10 columns are unacceptable. It is important to keep tables concise and easy to synthesize. Tables will be posted on-line as .jpg files 420 pixcels.
Appendixes
Appendixes with links in the text are encouraged for large amounts of data. Please indicate in the text where the link is to be placed.
Figures
Figures may be professionally designed or photographed. They should be saved (by scanning if necessary), as .jpg (preferred), .tiff, or Powerpoint (.ppt) formats at these resolutions: 1200 dpi for line art (e.g., graphs, drawings that have no gray tones), 300 dpi for black and white and color photographs with no labeling, and 600 dpi for combination figures (photographs with labeling). Figures will be posted on-line as .jpg files 420 pixels. Size is limited to GB.
Signed statements of consent to publish their image must accompany a photograph if there is a possibility the subject could be identified. If an image must be manipulated to show detail, the manipulation should be applied to the entire figure; it is not acceptable to adjust specific elements of a figure. Any manipulation to the figure must be disclosed and explained in the caption.
Movies
Southwest Journal of Pulmonary & Critical Care will publish movies. These should be submitted as either .gif (preferred), .swf, .avi, or QuickTime movies. Submission of movies for CT scans, ultrasound or echocardiography is encouraged. Size is limited to 20 GB. Signed statements of consent to publish their image must accompany a movie if there is a possibility the subject could be identified.
Supporting Material
Online-Only Material
Southwest Journal of Pulmonary & Critical Care accepts and publishes online-only material.
Permissions When use of tables and figures from copyrighted sources is necessary, authors should (1) obtain permission for all print, online, and licensed uses from the copyright holder (usually the publisher); (2) provide copies of the permission with their submissions (use “supplemental material” as the file type when uploading into Southwest Journal of Pulmonary & Critical Care; (3) acknowledge the source in the caption; (4) provide the full citation in the reference list; and (5) ensure that any language requirements of the copyright holder have been met (e.g., “Reproduced with permission from XXX”). If the copyright holders ask for payment, it is the responsibility of the authors to pay any fees.
If you use a PART of a table from a copyrighted article or book for a table in your submission, Southwest Journal of Pulmonary & Critical Care requires that you obtain permission from the copyright holder as if it were the entire table. Pieces of data are not copyrightable, but the formatting and summarizing of them are.
Proper Use of Survey Instruments/Questionnaires
Many papers submitted to Southwest Journal of Pulmonary & Critical Care are based on survey instruments/questionnaires. It is the responsibility of researchers to know if the survey instrument they use is copyrighted and, if so, to comply with the copyright terms. If a copyrighted survey instrument has been used, authors are responsible for receiving permission to use the survey from the copyright holders. It is generally unacceptable to adapt surveys, and especially unacceptable without the permission of the developer(s) of the survey. A copy of the permission to use a copyrighted survey must be attached with the manuscript submission (attach it as “supplemental material” in the file upload area). Surveys that have been translated must be validated and undergo a new psychometric analysis. Authors should confirm that a translated survey has been so validated.
Journal Sections
For a complete list of current sections for Southwest Journal of Pulmonary & Critical Care, see Table 1 below. Authors should review the information in these tables, because requirements differ among the various sections. For example, each section contains its own maximum length requirements.
Table 1. Current unsolicited sections of Southwest Journal of Pulmonary & Critical Care and maximum length requirements (As of August 2013).
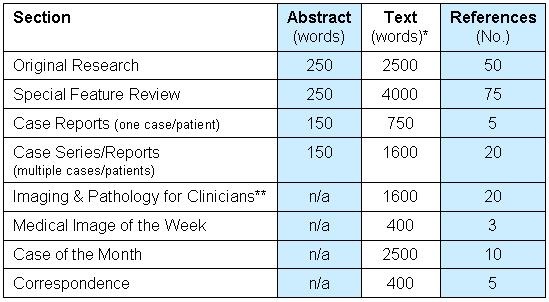
*Does not include title, abstract, or references. Refers to the body of the text.
**Approximate breakdown of the clinical, radiology, and pathology findings and discussion should be approximately 500 words. Whenever appropriate, plain chest radiographs should be included.
Those with questions should contact the Editor (rickrobbins@cox.net) before they begin to write. Southwest Journal of Pulmonary & Critical Care strongly discourages inquiries from anyone but the submitting author/principal investigator; inquiries and requests should not come from third-party medical writers and medical writing companies.
Correspondence
General: All Correspondence meant for publication should be submitted online to rickrobbins@cox.net (preferred), SWPCC@cox.net or via http://www.SWJPCC.com. When preparing the manuscript, use the standard Southwest Journal of Pulmonary & Critical Care format for the title page. While the correspondence section is primarily intended for clarification and edification of articles published in Southwest Journal of Pulmonary & Critical Care, letters that describe research in preliminary terms and announcements of general interest are also occasionally published.
Length: Letters in response to previously published articles should not exceed 400 words and 5 references; replies from authors should not exceed 400 words and 5 references (exceptions may be made if an author is replying to multiple letters on the same article), and announcement, general interest, and research letters should not exceed 400 words and 7 references. Only one table and one figure are permitted per letter. Supplemental material is acceptable in Correspondence if it adds to the contribution.
Peer Review: It is up to the discretion of the Editor in Chief whether any Correspondence is sent for external peer review and whether to accept any letter for publication.
Editing: Southwest Journal of Pulmonary & Critical Care reserves the right to edit letters for length, content, grammar, and style. Authors will be provided the opportunity to approve any changes.
Correspondence discussing recent Southwest Journal of Pulmonary & Critical Care articles: Any letter should include a short title that does not repeat the title of the article. Please include the article to which you are responding in the citations. For letters submitted regarding Papers in Press, Southwest Journal of Pulmonary & Critical Care will hold publication until the final version of the article is published. All accepted letters commenting on articles will be sent to the Corresponding Author of the original article with an invitation to respond. Letters commenting on articles should strive to provide constructive criticism of the work.
Correspondence in reply: Authors are asked to reply to letters on their work within four weeks of receipt of the invitation to reply. The title should be “Response.” Authors should never correspond directly with the authors of Correspondence regarding their work.
Correspondence of general interest and announcements: Southwest Journal of Pulmonary & Critical Care will consider Correspondence that serves to announce matters of importance to the medicine community. The letter should be exclusive to Southwest Journal of Pulmonary & Critical Care.
Comments
Comments may be added on-line at the bottom of each article. The comments should be relevant to the article. The comments are reviewed before posting. No comment will be considered without full names of the author. Southwest Journal of Pulmonary & Critical Care reserves the right to edit comments for length, content, grammar, and style.
Imaging Section
Clinicians in our field rely heavily on Southwest Journal of Pulmonary & Critical Care radiology and interpretation of images to determine diagnoses. To aid our readers in mastering the fundamentals of interpretation and ordering of Southwest Journal of Pulmonary & Critical Care imaging modalities, Southwest Journal of Pulmonary & Critical Care will regularly publish case-based articles with characteristic imaging and related pathology. The editors of this section will oversee and coordinate the publication of a core of the most important imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiology and pathology images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathology images. Taking pictures of plain radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Other requirements for manuscript submission are listed in the Instructions for Authors.
Special Instructions for Medical Image of the Week
There is no limit to the number of images submitted with each case. But, no more than 5 authors are permitted for any "Image of the Week" submission. No more than 3 references are permitted.
Case Presentation
The case should cover in sequence clinical findings, radiology findings, and pathology findings without the use of subheading and without giving away the diagnosis. Specific instructions for each of these is as follows:
Clinical Findings
Should briefly mention the pertinent positive and negatives. Any unnecessary investigations and detailed description of hospital course should be avoided.
Radiographic Findings
This discussion should usually begin with the plain Southwest Journal of Pulmonary & Critical Care radiograph when appropriate. With the advent of newer imaging modalities, plain Southwest Journal of Pulmonary & Critical Care radiograph interpretation is becoming an overlooked art. Normal Southwest Journal of Pulmonary & Critical Care radiographs, however, need not be submitted. A detailed description of additional imaging studies should be made. Subtle findings that help point towards the diagnosis should be emphasized. Clinicians should be able to suggest the correct diagnosis or a short differential based upon familiarity with the appearance of classic radiographic findings by themselves. Selection of images should reflect state-of-the-art image quality. For example, cases of interstitial lung disease must be imaged with high-resolution CT technique. Similarly, CT or MR studies related to vascular disease must be performed with contrast enhancement. Cases illustrating advanced imaging techniques such as volumetric rendered images, or virtual endoscopy are also welcome provided that these techniques prove critical to radiology diagnosis.
Pathology Findings
A detailed description of the pathology findings should be included. This section should be fairly detailed and should reflect whenever possible correlations with the above mentioned radiology signs.
Following the Case Presentation, please insert the following headings:
What is the diagnosis? Alternative questions may replace asking for the correct diagnosis when these represent a more challenging or informative method for introducing cases.
Discussion
The discussion must be divided into three broad areas with subheadings:
- Clinical discussion. How do the clinical findings tie in with the diagnosis? Mention the typical and atypical features of the case. Highlight the two or three clinical features that may alert the clinician to the correct diagnosis. A detailed description of the differential diagnosis and a logical approach to exclude them would be useful.
- Radiology discussion. Specific findings on plain Southwest Journal of Pulmonary & Critical Care radiographs and CT PET or MR scans should be highlighted. Radiographic findings that help exclude diagnoses or make them less likely should be mentioned. Finally, the reason(s) to select a particular imaging modality over another should be discussed.
- Pathology discussion. Pathology patterns of lung involvement that correspond to patterns seen on Southwest Journal of Pulmonary & Critical Care imaging and the pathology differential diagnosis of the disease under discussion should be presented. Special staining techniques that may allow the diagnosis to be established should be addressed.
A concluding paragraph should enumerate the patient’s clinical course and should mention the treatment given. Our aim is to give the readers condensed information about a particular disease, allow them to form a complete differential diagnosis, and to select imaging modalities that give the most useful information in a cost effective manner.
Special Instructions for Submission to the Transparency in Health Care Section
This section will publish papers that have studied an aspect of patient safety in an organized and scientific manner. Case series, and possibly case reports, may be acceptable if they include specific, generally applicable clinical teaching points. Thoughtful commentaries on patient safety and transparency in healthcare are encouraged. For word count and reference limits see Table 1.
Case Series/Reports
Focus: Papers should address patient safety and medical errors from a scientific, learning and teaching perspective. Papers should be clinically case based and focus on “medical errors” and “near misses” to illustrate important aspects of clinical care.
Focused case presentation: The case presentation should focus on the salient points of the case history. Specific patient identifiable information will not be presented. Minor demographic or clinical points may be omitted or modified to preserve patient identify. Identification of specific company products must be omitted.
Identified teaching point: Each case must contain at least one “take home” teaching point that will be generally applicable to the practice of cardio-respiratory medicine.
Error reduction strategy: Authors should identify the error reduction strategy that they implemented following the clinical event and the effectiveness of this strategy. Authors are encouraged to develop simulations of the medical error and make the simulations available for Internet download.
Protection of physician identity: Papers may be published under the author(s) name or using a nom de plume (true identify must be known to the editors in all cases). Institution can be identified or not at the author’s request. If requested, a confidential letter can be provided to the authors from the series editors, identifying the authors for academic recognition purposes.
Case of the Month
Interesting cases that include good teaching points or difficult diagnosis and/or treatment may be submitted for the Case of the Month series. These are published monthly in pulmonary, critical care, and imaging. The cases usually involve CME and are done in a question and answer case presentation style. The author will need to work closely with the editor in developing these cases for online presentation. Authors are advised to contact the editor before submission.