
Executive Pay and the High Cost of Healthcare
Two recent articles examined hospital executive pay. One was “Bitter Pill: Why Medical Bills Are Killing Us” from Time magazine (1). We reviewed this article in our “March 2013 Critical Care Journal Club” (2). The other is a more recent article from Kaiser Health News (3). The later is particularly intriguing since it discusses healthcare executive compensation. We thought it might be of interest to examine executive compensation from selected nonprofit hospital tax returns from Arizona, New Mexico and Arizona. (Table 1). [Editor's note: It may be necessary to enlarge the view on your browswer to adquately visualize the tables.]
Table 1. Financial information from Southwest hospitals latest year tax return as listed by GuideStar (4).
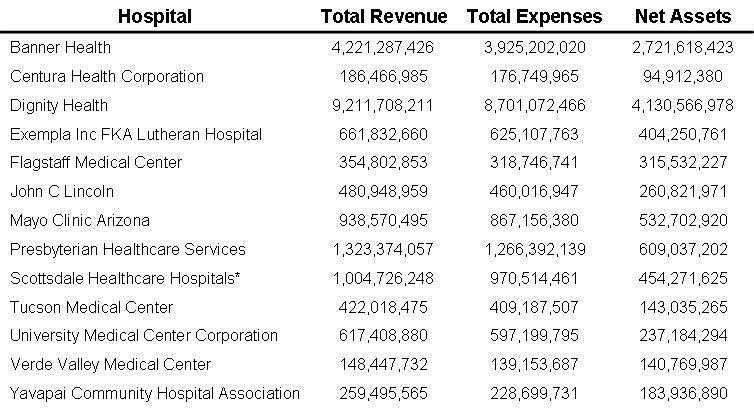
*Includes Scottsdale Healthcare Corporation
These Southwest hospitals appear to be doing quite well. Overall they had combined incomes of $19,831,088,546, assets of $ 10,228,640,923 and profits of $1,145,888,944. None lost money. Although the data from organizations such as Dignity, Banner, Scottsdale Healthcare, Exempla, and Presbyterian Healthcare include several hospitals, they are doing well, especially for “nonprofit” hospitals.
The CEOs were also doing well (Table 2).
Table 2. CEO and executive compensation from Southwest hospitals latest year tax return as listed by GuideStar (4).
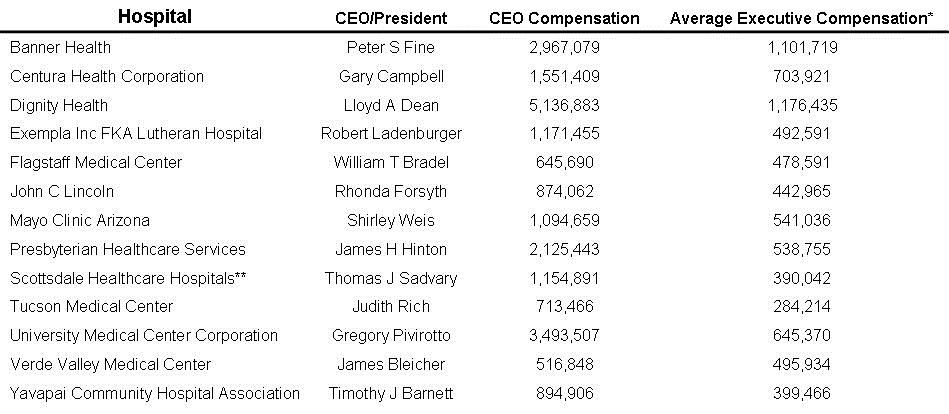
*Includes employees listed on Form 990.
**Includes Scottsdale Healthcare Corporation
The CEOs were paid an average of $1,718,484 and the average executive made $591,618. Not bad for being paid by a “nonprofit” organization. The CEO pay is nearly 8 times and the executive pay is nearly 3 times the slightly over $200,000 average Southwest pulmonary and critical care physician received in 2011 (5).
The Kaiser Healthcare News article went on to point out that boards at nonprofit hospitals are often paying hospital administrators much more for boosting volume than delivering healthcare value (3). Hospital administrators agreed but were quick to point out that compensation is increasingly being determined by healthcare performance incentives. However, James Guthrie, a hospital compensation consultant for Integrated Healthcare Strategies stated about administrative compensation, "What you're seeing is incentive plans that look pretty similar to what they looked like five years ago or ten years ago…they're changing, but they're changing fairly slowly."
Two of the local executives mentioned in the Kaiser Healthcare News article were Lloyd Dean and Peter Fine, heads of Dignity Health and Banner Health respectively. Incentive goals for Dean included unspecified "annual and long-term financial performance” (4). Dean's bonus for 2011 was $2.1 million. Fine speaks of "an unwavering commitment to improve clinical quality and efficiency" but Fine's long-term incentive goals included profits and revenue growth (4).
"Boards of trustees in health care are oriented around top-line, revenue goals," said Dr. Donald Berwick, who was CEO of the Institute of Healthcare Improvement (IHI) and later the Administrator for the Centers for Medicare and Medicaid Services (CMS) (Figure 1).

Figure 1. Dr. Donald Berwick
"They celebrate the CEO when the hospital is full instead of rewarding business models that improve patients' care." Such deals undermine measures in the 2010 health law that aim to cut unnecessary treatment and control costs, say economists and policy authorities (3).
An explosion of medical regulatory groups have arisen to improve quality, including Berwick’s IHI. These regulatory groups have often produced guidelines embraced by hospital administrators as improving healthcare. However, the administrators are often self-servingly paid bonuses for guideline compliance. Because nearly all the regulatory organizations are “nonprofit” like the hospitals, surely they would have more modest profits (Table 3).
Table 3. Financial information of healthcare regulatory organizations from latest year tax return as listed by GuideStar (4).
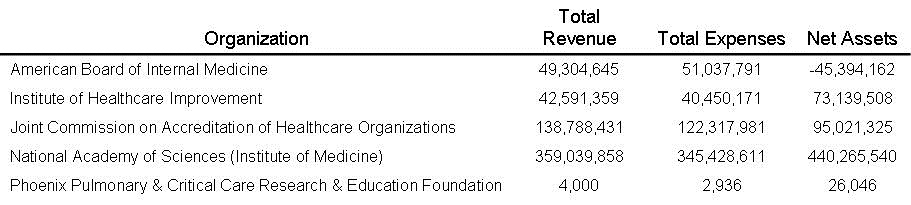
We are happy to report that the regulatory organizations had much more humble finances compared to the Southwest hospitals. Overall the four we examined totaled incomes of $589,724,293, assets of $563,032,211 and profits of $30,489,739. Only the American Board of Internal Medicine lost money with a loss of $-1,733,146 on income of nearly $50 million. For comparison, we added the Phoenix Pulmonary and Critical Care Research and Education Foundation to Table 3. It is the financial source behind the Southwest Journal of Pulmonary and Critical Care.
Executive pay was also more modest than Southwest hospital administrators (Table 4).
Table 4. CEO and executive compensation from healthcare regulatory organizations latest year tax return as listed by GuideStar (4).
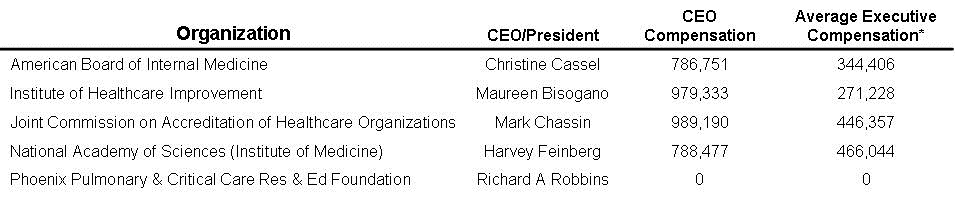
*Includes employees listed on Form 990.
The CEOs were paid an average of $885,938 and the average executive made $382,009. Although much lower than the average $1,718,484 and the $591,618 paid to Southwest hospital CEO and executives, these salaries are still not bad for a “nonprofit” organization.
The only regulatory organization to lose money was the American Board of Internal Medicine. Either an increase or revenue or a decrease in expenses will eventually be necessary. The major source of income for the American Board is test revenue and increasing the fee for certification or the frequency and/or fees for maintenance of certification may be necessary. Alternatively, they could pay their CEO less than $786,751, eliminate the CEO’s spousal travel benefits, or lower the compensation for general internists such as Eric Holmboe from $417,945 to be more in line with the $161,000 average income of general internists in the mid-Atlantic region (4,5).
Donald Berwick has a good point and is correct. Hospital administrators need to be rewarded more for improving healthcare and less for keeping the hospital full and profits high. However, in 2009 while CEO at IHI Berwick was compensated $920,952 (4). This is almost 7 times the compensation of the average pediatrician in New England (5). Included were $88,200 in bonuses. It is unclear from the tax return what justified these bonuses (4).
Executive pay for both hospital and regulatory administrators is too high and contributes to the high cost of healthcare. We find no evidence that either type of administrator contributes much to improved patient-centered outcomes. Quality care continues to rely on an adequate number of good doctors, nurses and other healthcare providers. If anyone should be paid bonuses for healthcare, it is those providing care, not administrators.
Present bonus systems for healthcare administrators are perverse. As noted above these include bonuses for keeping the hospital full and profits high, neither consistent with what should be the goals of a nonprofit organization. Furthermore, increasing pay for supervising an increased number of administrative personnel will only add to the increasing costs. If administrators must be paid a bonus let them be paid for performance directly under their control. This could include ensuring that adequate numbers of good doctors and nurses are caring for the patients and improving administrative efficiency. These should result in better care but lower numbers of administrators consuming fewer healthcare dollars.
Last Friday, June 14, the Medicare Payment Advisory Commission, or MedPAC released their recommendations to Congress (8). These include recommendations that may be relative to hospital administrative pay. One is for “site-neutral payment”. Currently Medicare pays hospitals more than private physician offices for many services. MedPAC recommended that Congress “move immediately to cut payments to hospitals for many services that can be provided at much lower cost in doctors’ offices.” The commission said that “current payment disparities had created incentives for hospitals to buy physician practices, driving up costs...” This will increase the hospital’s bottom line, and therefore, the administrators’ bonuses. We agree with MedPAC’s recommendation.
MedPAC also told Congress that “the financial penalties that Medicare imposes on hospitals with high rates of patient readmissions are too harsh for hospitals serving the poor and should be changed.” Based on this and data that higher mortality is associated with lower readmission rates, we agree (9). Rewarding hospitals for potentially harmful patient practices that increase the hospital’s bottom line are not appropriate. Financial incentives for reducing readmissions should only be part of a more global assessment of patient outcomes including mortality, length of stay and morbidity. Regulatory administrators need to become more focused on patients and less on an endless array of surrogate markers that have little to do with quality of care.
Richard A. Robbins, M.D.*
Clement U. Singarajah, M.D.*
References
- Brill S. Bitter Pill: Why Medical Bills Are Killing Us. Time. February 20, 2013. PDF available at: http://livingwithmcl.com/BitterPill.pdf (accessed 6/17/13).
- Stander P. March 2013 critical care journal club. Southwest J Pulm Crit Care. 2013;6(4):168-9. Available at: http://www.swjpcc.com/critical-care-journal-club/2013/4/2/march-2013-critical-care-journal-club.html (accessed 6-17-13).
- Hancock J. Hospital CEO Bonuses Reward Volume And Growth. Kaiser Health News. June 16, 2013. Available at: http://www.kaiserhealthnews.org/Stories/2013/June/06/hospital-ceo-compensation-mainbar.aspx (accessed 6-17-13).
- http://www.guidestar.org/ (accessed 6-17-13).
- http://www.medscape.com/sites/public/physician-comp/2012 (accessed 6-17-13).
- Robbins RA, Thomas AR, Raschke RA. Guidelines, recommendations and improvement in healthcare. Southwest J Pulm Crit Care 2011;2:34-37. Available at: http://www.swjpcc.com/editorial/2011/2/25/guidelines-recommendations-and-improvement-in-healthcare.html
- Robbins RA. Why is it so difficult to get rid of bad guidelines? Southwest J Pulm Crit Care 2011;3:141-3. Available at: http://www.swjpcc.com/editorial/2011/11/1/why-is-it-so-difficult-to-get-rid-of-bad-guidelines.html
- http://www.medpac.gov/documents/Jun13_EntireReport.pdf (accessed 6-17-13).
- Robbins RA, Gerkin RD. Comparisons between Medicare mortality, morbidity, readmission and complications. Southwest J Pulm Crit Care. 2013;6(6):278-86. Available at: http://www.swjpcc.com/general-medicine/2013/6/13/comparisons-between-medicare-mortality-readmission-and-compl.html
*The opinions expressed are those of the authors and not necessarily the Southwest Journal of Pulmonary and Critical Care or the Arizona, New Mexico or Colorado Thoracic Societies.
Reference as: Robbins RA, Singarajah CU. Executive pay and the high cost of healthcare. Southwest J Pulm Crit Care. 2013;6(6):299-304. doi: http://dx.doi.org/10.13175/swjpcc080-13 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.