
Medical Image of the Month: Bleomycin-Induced Pulmonary Fibrosis in a Patient with Lymphoma
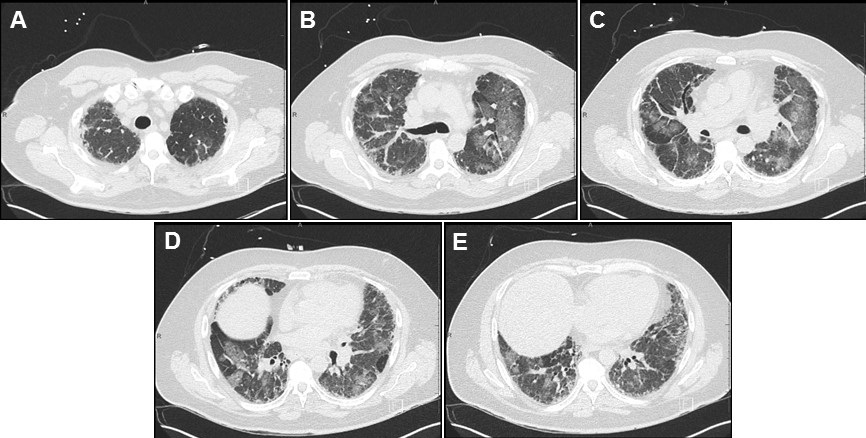
Figure 1. Representative images from the thoracic CT in lung windows showing scattered bilateral ground glass opacities with areas of fibrosis consistent with multifocal pneumonia superimposed on pulmonary fibrosis.

Figure 2. Representative image from the thoracic CT in lung windows done just prior to lung transplantation.
Abstract
Interstitial pulmonary fibrosis is the most feared complication of bleomycin therapy and occurs in up to ten percent of patients that receive the drug. The risk of bleomycin-induced pulmonary fibrosis is related to the age of the patient, the dose of medication given, the patient’s kidney function, and whether the patient smokes cigarettes. Current screening guidelines for bleomycin-induced lung injury are limited, but most clinicians screen high risk and symptomatic patients with pulmonary function testing. This case report is of a patient with lymphoma who received bleomycin as a part of his chemotherapy regimen, and later developed pulmonary fibrosis complicated by bouts of eosinophilic multifocal pneumonia. The case highlights the importance of close monitoring of patients taking bleomycin for signs and symptoms of pulmonary fibrosis and the need for major medical societies to issue concrete screening guidelines.
Introduction
Bleomycin’s labeled indications include treatment of squamous cell carcinomas of the head and neck, Hodgkin lymphoma, non-Hodgkin lymphoma, malignant pleural effusions, and testicular cancer (1). The most feared complication of bleomycin is interstitial pulmonary fibrosis (2). Pathogenesis is not fully clear but involves oxidative damage secondary to reactive oxygen species (2). Risk factors include age > 40, renal insufficiency (CrCl < 80 mL/min), bleomycin dose > 300 units, and cigarette smoking (2). Symptoms present within one to six months of starting the medication and often begin with dyspnea and auscultatory crackles on physical exam (2). Associated signs and symptoms include cough, chest pain, opacities on chest radiographs, or an asymptomatic decline in diffusing capacity for carbon monoxide (2,3).
Screening for pulmonary fibrosis in patients taking bleomycin is controversial and no clear guidelines exist. Most physicians agree that it is appropriate to get baseline pulmonary function tests (PFTs) in patients receiving bleomycin, and thereafter screen with PFTs intermittently throughout the course of treatment (3). FDG-PET has also been used as a screening tool, but the evidence for its efficacy is mixed (4).
This is a case of a 56-year-old man with a presumed diagnosis of multifocal eosinophilic pneumonia superimposed on pulmonary fibrosis who had to be admitted to the ICU for respiratory distress. The patient recovered and underwent a lung transplant.
Case Presentation
A 56-year-old man with a history of lymphoma diagnosed 11 years prior and treated with chemotherapy, including bleomycin, presented to the emergency department with fever, chills, and productive cough. A CT of the chest with IV contrast was performed which revealed scattered bilateral ground glass opacities with areas of fibrosis (Figure 1). Next, the patient underwent a bronchoalveolar lavage (BAL) and shortly thereafter developed respiratory distress with respiratory failure that required non-invasive ventilation and admission to the ICU. In the ICU, the patient responded to ceftriaxone, azithromycin, prednisone, and fluconazole. The bronchoalveolar lavage was significant for elevated levels of eosinophils and neutrophils. There were also possible fungal elements on touch prep but no fungal growth. The presumed diagnosis on admission was multifocal pneumonia superimposed on pulmonary fibrosis.
After recovering, the patient was discharged. Four months later, he underwent a bilateral lung transplant. At explant, the final pathology report confirmed a mixed pattern of fibrosing interstitial lung disease, clinically due to bleomycin. Figure 2 shows the patient’s pulmonary fibrosis just prior to transplant.
The patient’s lung transplantation was successful, and he is currently doing well.
Discussion
Pulmonary fibrosis is a dangerous and relatively common complication of bleomycin. The differential diagnosis includes pulmonary infection, cardiogenic pulmonary edema, radiation-induced pulmonary fibrosis, metastatic disease, and adverse reaction to other medications. Presented here is a case where a patient received bleomycin as a part of his chemotherapy regimen for lymphoma, and subsequently developed pulmonary fibrosis. When the patient presented 11 years after his lymphoma diagnosis, he had eosinophilic multifocal pneumonia superimposed on his already existing pulmonary fibrosis.
This case illustrates the difficulty of managing the pulmonary manifestations of bleomycin in patients taking the drug. There are currently no screening guidelines in place for patients that take the medication (3). Shippee et al. suggest patients undergo PFTs at baseline before starting treatment, followed by PFTs every 3 weeks during therapy (3). They suggest bleomycin should be discontinued in patients who have a linear decline in DLCO of 40-60% from baseline (3).
It is unclear if our patient had been screened for pulmonary fibrosis while he was receiving bleomycin. Regardless, it would be prudent and appropriate for a major medical society to issue clear guidelines regarding screening for pulmonary fibrosis. Standardizing screening protocols will lead to better patient outcomes.
Martin A. Dufwenberg, BS
University of Arizona College of Medicine – Tucson
Tucson, AZ, USA
Acknowledgments
The author thanks Dr. Michael Larson, M.D., Ph.D., for mentorship, discussion, and help in making this case report become reality.
References
- U.S. Food and Drug Administration. Blenoxane (bleomycin sulfate for injection, USP). Updated April 2010. Accessed June 8, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001 Aug;120(2):617-24. [CrossRef] [PubMed]
- Shippee BM, Bates JS, Richards KL. The role of screening and monitoring for bleomycin pulmonary toxicity. J Oncol Pharm Pract. 2016 Apr;22(2):308-12. [CrossRef] [PubMed]
- Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, Kayani I, Menezes LJ, Dickson JC, Ell PJ. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18F-FDG PET/CT. J Nucl Med. 2009 Apr;50(4):538-45. [CrossRef] [PubMed]
Cite as: Dufwenberg MA. Medical image of the month: bleomycin-induced pulmonary fibrosis in a patient with lymphoma. Southwest J Pulm Crit Care. 2021;23(2):49-51. doi: https://doi.org/10.13175/swjpcc024-21 PDF
 Post a Comment
Post a Comment