
August 2023 Medical Image of the Month: Cannonball Metastases from Metastatic Melanoma
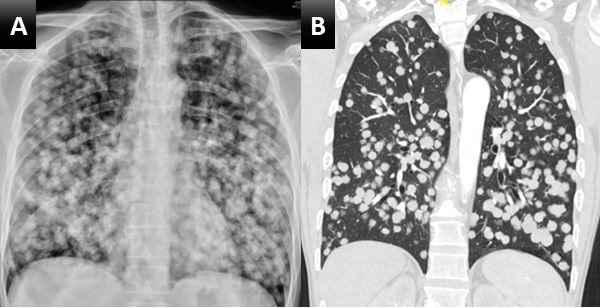 Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
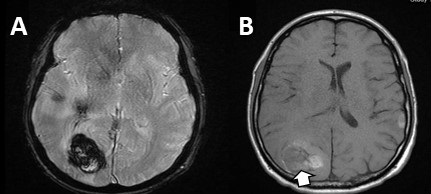 Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
A 48-year-old man with a significant smoking history presented with progressive dyspnea, a mildly productive cough with brown-tinged sputum, headache, weight loss, and progressive back pain over a period of 8 weeks. The patient had no known history of lung conditions. As part of their initial evaluation, the patient received a frontal CXR and was found to have innumerable rounded pulmonary nodules throughout the lungs, which were consistent with a “cannonball” pattern of pulmonary metastatic disease (Figure 1A). A subsequent CT confirmed innumerable pulmonary metastases (Figure 1B). An MRI of the brain and spine revealed hemorrhagic brain metastases (Figure 2), spinal metastases, and bone metastases. A biopsy of a lesion in the left iliac bone confirmed the diagnosis of metastatic melanoma.
This case highlights the so-called “cannonball” pattern of pulmonary metastatic disease with innumerable round nodules throughout the lungs with a slight lower lung predilection, consistent with a hematogenous spread of disease to the lungs. Classically, this pattern consists of numerous well-circumscribed relatively large lesions in the lungs with a pattern resembling multiple small "cannonballs". The distribution of nodules is random, and the factors that distinguish a cannonball pattern from a miliary pattern of pulmonary metastatic disease are that cannonball metastases are larger and less numerous compared to a miliary pattern of pulmonary metastatic disease (1,2). Although cannonball pattern of pulmonary metastatic disease is classically described in the setting of metastatic renal cell carcinoma, prostate cancer, choriocarcinoma, and sarcoma, it has been reported for a variety of other primary cancers, including melanoma. Similar cases of late-stage metastatic melanoma presenting as widely metastatic disease of unknown origin has also been reported (3).
Melanoma spreads to the lungs through hematogenous dissemination, resulting in the cannonball (or miliary) lesions observed on imaging. Specifically, when these lesions are small and distributed throughout the lung, they commonly indicate metastatic melanoma. While this classical presentation can be pathognomonic, it is important to consider other potential diagnoses, including malignancy, infectious diseases, and rheumatologic conditions. Malignant causes encompass metastatic colorectal cancer, breast cancer, renal cell carcinoma, choriocarcinoma, prostate carcinoma, and adrenal carcinoma. Additionally, non-cancerous causes include infectious etiologies such as septic emboli, coccidiomycosis, histoplasmosis, miliary tuberculosis, and nocardiosis. It is also important to note that rheumatologic conditions like granulomatosis with polyangiitis (Wegener's granulomatosis) can present with the cannonball sign; however, they typically involve both the upper and lower lungs. In this case, the lesions were determined to be due to metastatic melanoma, which had spread to the lungs via hematogenous dissemination.
For this patient, an oncologist was consulted, who recommended that the patient undergo treatment with ipilimumab and nivolumab. The response rate for this treatment regimen generally exceeds 50%, and more than 50% of individuals continue to survive after 5 years. Frequently, when extensive metastases are observed on imaging, healthcare providers often assume a limited life expectancy and tend to lean towards discussions of hospice care. However, it is important to keep in mind that even in cases of extensive metastatic disease, many cancers can be effectively treated with novel and highly effective immunologic anticancer medications.
Andrew Barsoum MD, Mueez Hussain MD, Ranjit Sivanandham MD, and Sina Bagheri MD.
Southwest Healthcare System
Murrieta, California
References
- Ammannagari N, Polu V. 'Cannon ball' pulmonary metastases. BMJ Case Rep. 2013 Jan 8;2013:bcr2012008158. [CrossRef][PubMed]
- Andreu J, Mauleón S, Pallisa E, Majó J, Martinez-Rodriguez M, Cáceres J. Miliary lung disease revisited. Curr Probl Diagn Radiol. 2002 Sep-Oct;31(5):189-97. [PubMed]
- Lowe A, Bray JJH. Late-stage melanoma presenting with cannonball metastases. BMJ Case Rep. 2020 Dec 12;13(12):e237969. [CrossRef][PubMed]
 Post a Comment
Post a Comment
Reader Comments