
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma
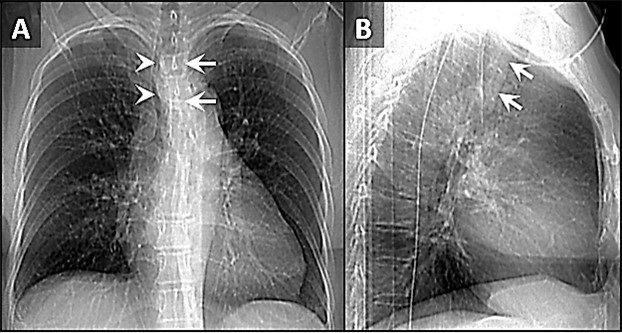
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
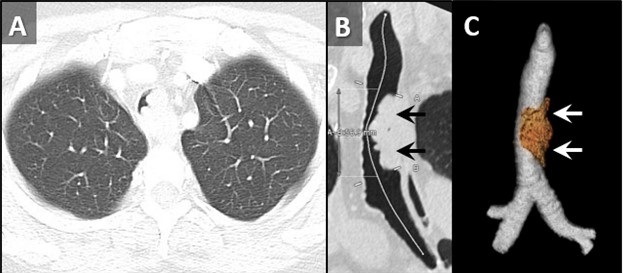
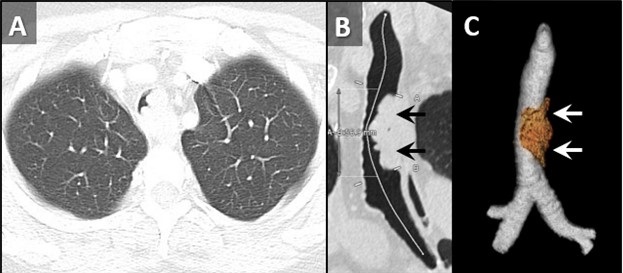
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
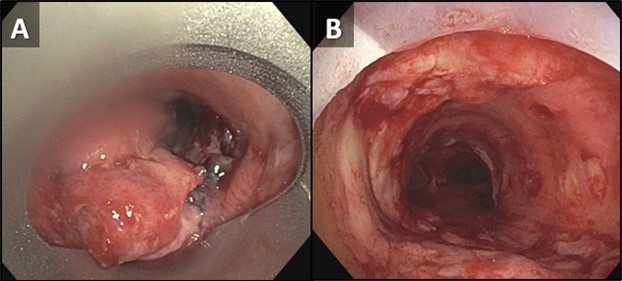
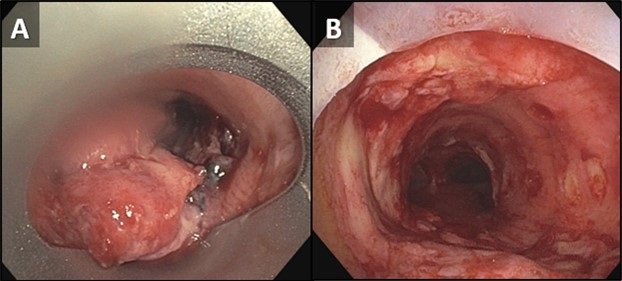
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
 Post a Comment
Post a Comment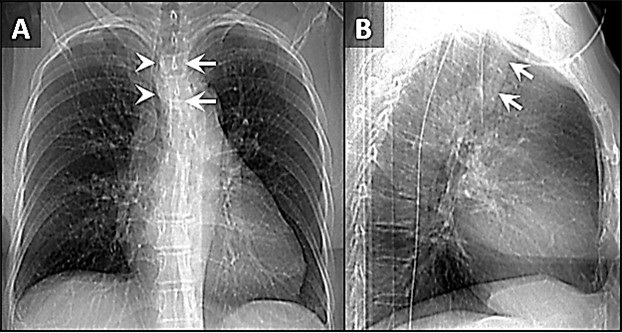{kind=link}
{kind=link}
{kind=link}
Reader Comments