
Medical Image of the Month: An Unexpected Cause of Chronic Cough
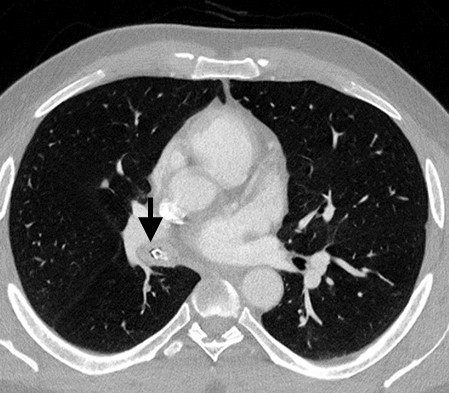
Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).
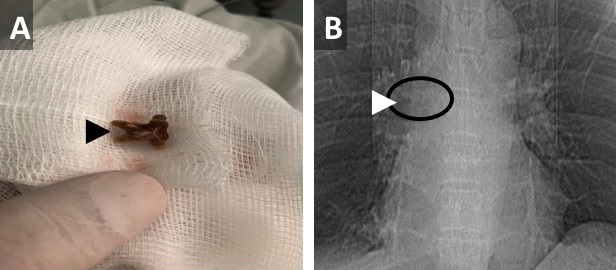
Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF
 Post a Comment
Post a Comment
Reader Comments