
April 2022 Medical Image of the Month: COVID Pericarditis
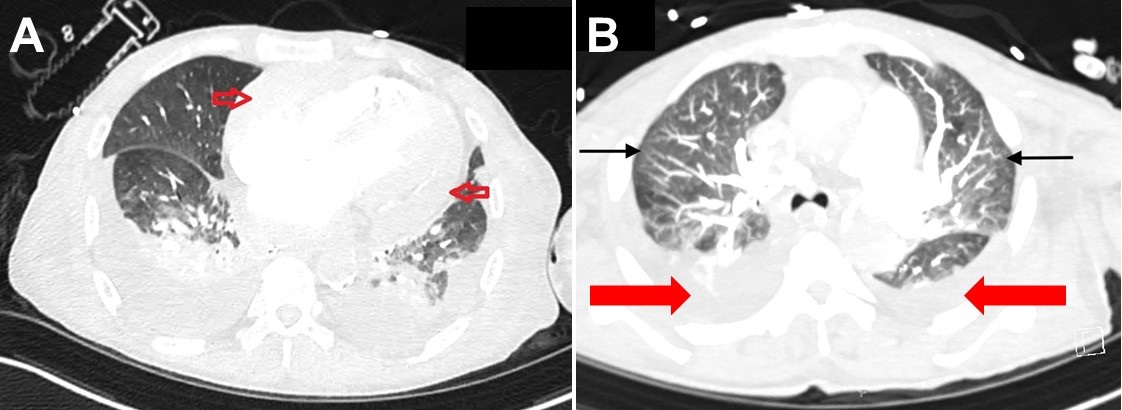
Figure 1. A: Pericardial enhancement on thoracic CT (red arrows). B: Thoracic CT in lung windows showing mosaic attenuation (black arrows) and bilateral pleural effusions (red arrows).
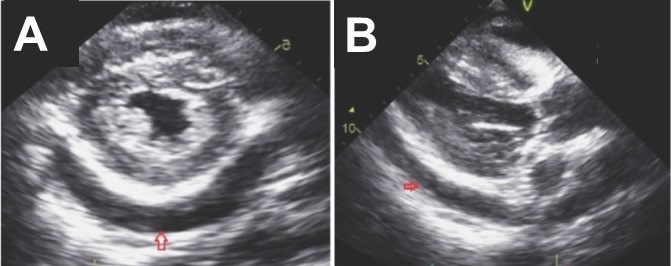
Figure 2. A: Static image of parasternal short axis on transthoracic echocardiogram showing moderate, generalized pericardial effusion with right ventricular diastolic collapse (red arrow). B. Static image of parasternal long axis on transthoracic echocardiogram again showing a moderate, generalized pericardial effusion (red arrow). Lower panel: video of echocardiogram in parasternal long axis view.
A 76-year-old patient presented with fatigue and shortness of breath after missing one session of dialysis. Past medical history included end stage renal disease on hemodialysis and atrial fibrillation on anticoagulation. Initial labs showed that she was COVID positive with mild elevation in troponin and a BNP 1200. While an inpatient, she had received a few sessions of dialysis and treatment for COVID (including dexamethasone and remdesivir). Initial echo showed an ejection fraction of 60-65% with a small generalized pericardial effusion, a thickened pericardium with calcification. A few days after admission patient was suddenly noted to be hypotensive with systolic blood pressure in the 70s and altered mental status. Repeated labs showed a D-Dimer of 17,232, leukocytosis, lactic acidosis, troponin 0.556 ng/ml and arterial blood gas with metabolic acidosis. With a worsening clinical picture, repeat imaging was obtained. CT angiography of the chest was negative for pulmonary embolism; however, it showed a large pericardial effusion with reduced size of the right ventricle more so than left, concerning for cardiac tamponade (Figure 1A). CT chest also showed moderate-to-large pleural effusions with scattered mosaic attenuation of the lung parenchyma (Figure 1B). Repeat transthoracic echocardiogram had a moderate generalized pericardial effusion with right ventricular diastolic collapse concerning for pericardial tamponade (Figure 2). Her airway was secured with endotracheal intubation and vasopressors added for hemodynamic support. Pericardiocentesis was indicated however, patient’s INR was severely elevated in the setting of anticoagulation use. Efforts were made to lower INR with FFP; however, patient had a PEA arrest the following day and expired.
COVID-19 has been classically known for its detrimental lung damage; however, it has shown to cause extrapulmonary effects as well. Cardiac injury is one phenomenon that has been seen with the fulminant inflammatory state that COVID is known to cause. With a few cases reported for COVID pericarditis, it is a possible culprit when all other causes have been ruled out. Pericardial involvement can be seen in about 20% of COVID 19 cases, with effusion found in about 5% of patients (1). Concomitant myocarditis can also be found in up to 17% of patients. Having isolated cardiac involvement with COVID is rare, with most cases presenting mainly as lung involvement in addition to other organs affected as well. Clinically, patients with pericarditis typically experience chest pain and in the setting of COVID infection, an increase in inflammatory markers. Characteristic findings of pericarditis include friction rub on auscultation, diffuse ST elevations on EKG and a potential progression to pericardial effusion on echo. When a pericardial effusion becomes large enough, it can progress to cardiac tamponade (2). Having a high clinical suspicion for tamponade is crucial in a patient who has developed respiratory distress and hypotension in the setting of recent viral pericarditis. It is a clinical diagnosis and requires rapid treatment with pericardiocentesis to prevent cardiac arrest.
Sarah Youkhana, MD1 and Maged Tanios, MD2
St. Mary Medical Center, Long Beach, CA USA
1Internal Medicine Resident, PGY-3
2Medical Director, Critical Care Services
References
- Diaz-Arocutipa C, Saucedo-Chinchay J, Imazio M. Pericarditis in patients with COVID-19: a systematic review. J Cardiovasc Med (Hagerstown). 2021 Sep 1;22(9):693-700. [CrossRef] [PubMed]
- Imazio M, Gaita F, LeWinter M. Evaluation and Treatment of Pericarditis: A Systematic Review. JAMA. 2015 Oct 13;314(14):1498-506. [CrossRef] [PubMed]
 Post a Comment
Post a Comment
Reader Comments