
August 2025 Medical Image of the Month: Crazy Paving in a Case of Eosinophilic Granulomatosis with Polyangiitis
 Figure 1. Axial reconstructions from a non-contrast chest CT at the level of the mid-lungs demonstrating patchy bilateral ground glass opacities which are superimposed upon underlying smooth septal line thickening. Findings are consistent with a “crazy paving” pattern of mixed interstitial and airspace disease. “Crazy paving” has a striking appearance on imaging, but is a relatively nonspecific finding on CT. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Axial reconstructions from a non-contrast chest CT at the level of the mid-lungs demonstrating patchy bilateral ground glass opacities which are superimposed upon underlying smooth septal line thickening. Findings are consistent with a “crazy paving” pattern of mixed interstitial and airspace disease. “Crazy paving” has a striking appearance on imaging, but is a relatively nonspecific finding on CT. To view Figure 1 in a separate, enlarged window click here.
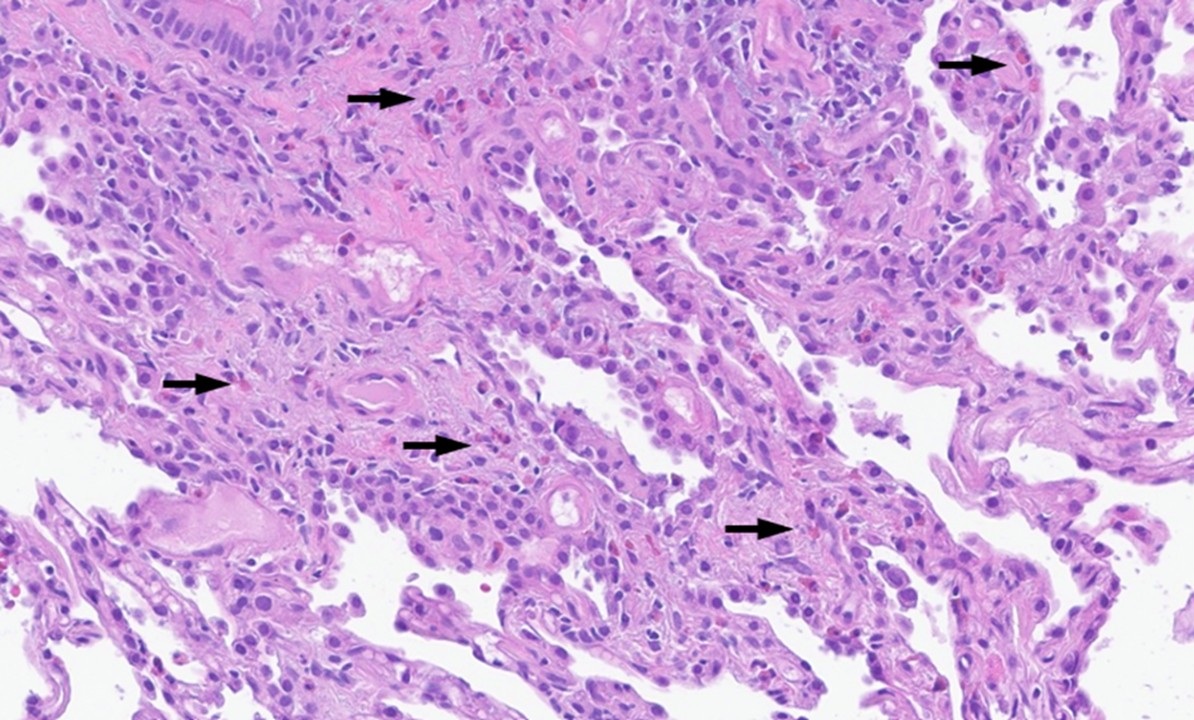
 Figure 2. Low-power H&E stain of pulmonary cryobiopsy specimen demonstrating chronic bronchitis with patchy airway-centered interstitial fibrosis with scattered non-necrotizing submucosal and interstitial granulomas with giant cells and scattered eosinophils (arrows). Findings could fit with EGPA but are considered nonspecific based on pathological findings alone. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Low-power H&E stain of pulmonary cryobiopsy specimen demonstrating chronic bronchitis with patchy airway-centered interstitial fibrosis with scattered non-necrotizing submucosal and interstitial granulomas with giant cells and scattered eosinophils (arrows). Findings could fit with EGPA but are considered nonspecific based on pathological findings alone. To view Figure 2 in a separate, enlarged window click here.
A 73-year-old woman with a history of eosinophilic granulomatosis with polyangiitis (EGPA), and heart failure with preserved ejection fraction presented to the hospital with acute pancreatitis and developed acute (on-chronic) hypoxic respiratory failure during treatment. Her previous EGPA complications included interstitial lung disease (ILD) as well as GI, skin, and cardiac involvement. She was being treated with rituximab and mepolizumab at the time of admission. However, this treatment had not improved her skin rashes, late-onset asthma, or arthralgias.
At admission, the patient was on a baseline of 3L oxygen, which worsened to 7-12L upon beginning IV fluids. The patients' labs were pertinent for B-type natriuretic peptide (BNP) 9378 pg/ml (normal <100pg/ml, increased from ~2000 2-months prior), lipase 702 U/L (normal , 0-160) and an absolute eosinophil count of 390cells/µL (normal 0-500). The transthoracic echocardiogram results were unchanged from four months prior, and diuresis failed to improve oxygen needs, raising the suspicion for an infectious/inflammatory etiology. Chest CT (Figure 1) showed patchy bilateral ground glass superimposed upon smooth septal line thickening, a “crazy paving” pattern of pulmonary involvement concerning for chronic eosinophilic pneumonia (CEP) vs organizing pneumonia vs EGPA flare. Bronchoscopy for BAL was deferred due to the patient’s condition. Infectious workup returned negative. A lung biopsy (Figure 2) showed interstitial fibrosis, granulomas with giant cells, and scattered eosinophils.
A rheumatology consult recommended a steroid trial, under the impression that this was a vasculitic/inflammatory condition. Although the patient’s Anti-Neutrophil Cytoplasmic Antibodies (ANCA) studies returned negative, she improved with oral prednisone 60 mg. This treatment response, along with imaging and pathologic studies suggests the most likely etiology to be an EGPA flare.
Eosinophilic granulomatosis with polyangiitis (EGPA), previously called Churg-Strauss syndrome, is a hypereosinophilic vasculitic disorder that presents with allergic manifestations such as asthma/obstructive lung disease, rhinitis, and peripheral blood eosinophilia. Additionally, clinical manifestations commonly involve the heart, lungs, sinuses, skin, and peripheral nerves; however, EGPA can involve almost any organ system (1,2). Unfortunately, EGPA can be clinically difficult to diagnose and differentiate from similar syndromes (3,4). Without proof of vasculitides in biopsy, most classification criteria struggle to differentiate EGPA from other eosinophilic disorders, and vasculitides may not develop until 8-10 years after initial allergic presentation. If biopsies are negative for vasculitis, a presumptive diagnosis can still be made based on peripheral eosinophilia and clinical findings after excluding alternative diagnosed (1).
On imaging, pulmonary manifestations of EGPA can be difficult to differentiate from other eosinophilic disorders, such as chronic eosinophilic pneumonia (CEP); however, there can be some differences. Although both EGPA and CEP commonly have bronchial wall thickening and bronchiectasis on HRCT, EGPA is more likely to have migratory lobular consolidations versus the homogenous peripheral airspace consolidations typical of CEP (3). This distinction can be important to make, as although first line agents for both conditions are glucocorticoids, the therapeutic strategies to treat end organ injury differ between CEP and EGPA (4). “Crazy Paving”, as was seen in this case, can be a very nonspecific finding on CT, associated with a variety of potential underlying disease processes (5,6). Early identification of EGPA from severe asthma, CEP, or other hypereosinophilic syndromes help guide effective treatment.
Jacob C. Wengler MS2 1 and Clint Jokerst, MD 2
1Mayo Clinic Alix School of Medicine,
2Department of Radiology,
Mayo Clinic Arizona
Phoenix, Arizona USA
References
- Khoury P. Clinical features and diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA) - UpToDate. https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-eosinophilic-granulomatosis-with-polyangiitis-egpa Updated 2025. Accessed Jul 18, 2025.
- Khoury P. Eosinophilic granulomatosis with polyangiitis: Treatment and prognosis - UpToDate. https://www.uptodate.com/contents/eosinophilic-granulomatosis-with-polyangiitis-treatment-and-prognosis Updated 2025. Accessed Jul 18, 2025.
- Jeong YJ, Kim KI, Seo IJ, Lee CH, Lee KN, Kim KN, Kim JS, Kwon WJ. Eosinophilic lung diseases: a clinical, radiologic, and pathologic overview. Radiographics. 2007 May-Jun;27(3):617-37; discussion 637-9. [CrossRef] [PubMed]
- Roufosse F. Hypereosinophilic syndromes: Clinical manifestations, pathophysiology, and diagnosis - UpToDate. https://www.uptodate.com/contents/hypereosinophilic-syndromes-clinical-manifestations-diagnosis-and-classification Updated 2022. Accessed Jul 18, 2025.
- Lin X, Lin Y, Lai Z, Wei S, Qiu M, Li J, Liu Q, Chung KF, Zeng Q, Zhang Q. Retrospective comparison of high-resolution computed tomography of eosinophilic granulomatosis with polyangiitis with severe asthma. Ann Transl Med. 2021 Jun;9(12):983. [CrossRef] [PubMed]
- Rossi SE, Erasmus JJ, Volpacchio M, Franquet T, Castiglioni T, McAdams HP. "Crazy-paving" pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics. 2003 Nov-Dec;23(6):1509-19. [CrossRef] [PubMed]
 Post a Comment
Post a Comment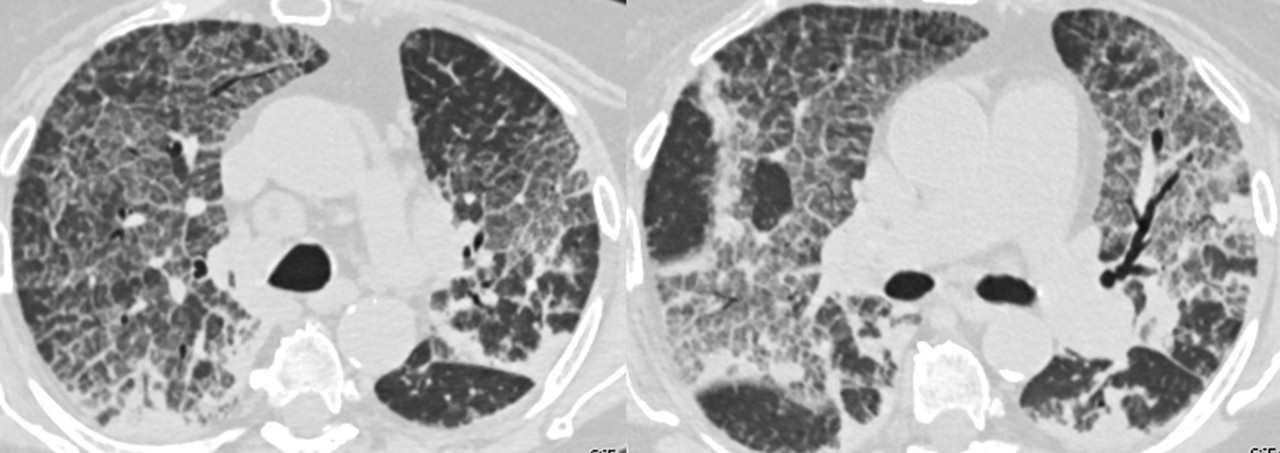{kind=link}
{kind=link}
Reader Comments