March 2024 Medical Image of the Month: Sputum Cytology in Patients with Suspected Lung Malignancy Presenting with Acute Hypoxic Respiratory Failure
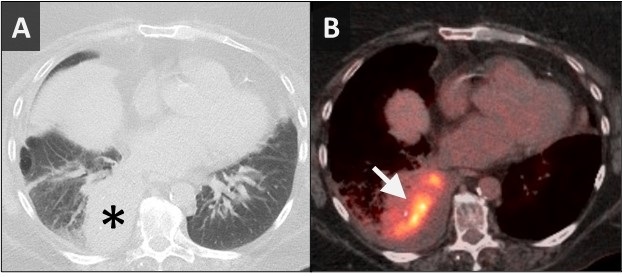 Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
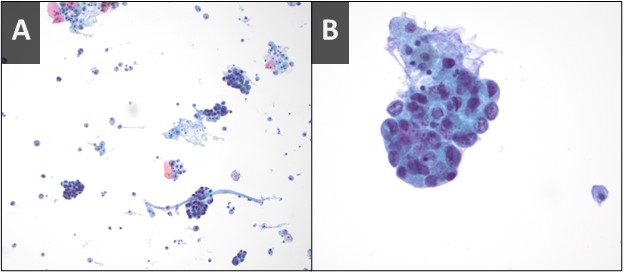 Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
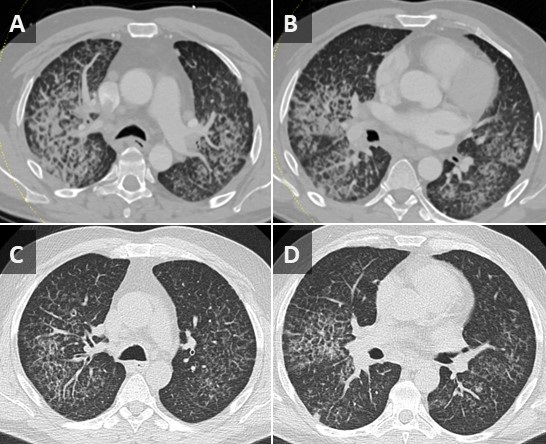
A 71-year-old woman presented with right-sided mass-like consolidation and pleural effusion on CT (Figure 1A), discovered incidentally after placement of a drug-eluting stent for coronary artery disease. The patient had a medical history significant for COPD, hypertension, hyperlipidemia, and coronary artery disease, status post a recent drug-eluting stent (less than 1 month ago). The patient received a presumptive diagnosis of pneumonia with parapneumonic effusion. Findings persisted despite multiple courses of empiric antibiotic therapy. She then underwent thoracentesis; pleural fluid was exudative; however, cytology was inconclusive. An FDG PET-CT (Figure 1B) revealed hypermetabolic activity in the right lower lobe with radiotracer activity up to 7.7 SUV concerning for malignancy. Diagnostic bronchoscopy was planned; however, her condition deteriorated suddenly the day before her planned procedure. EMS found the patient to be severely hypoxic, SpO2 in the 70s. Patient was taken by ambulance to the local emergency room.
Upon arrival, the patient was in mild respiratory distress which improved upon applying non-invasive positive-pressure ventilation. She had mild tachycardia and reduced air movement in the right lower third of the chest on physical exam. Repeat CT confirmed the persistence of the right lower lobe mass-like consolidation and moderate-sized pleural effusion. Empirical treatment for post-obstructive pneumonia was initiated. Right-sided thoracentesis again demonstrated exudative pleural fluid with negative cytology for malignancy and negative culture results. Due to concerns about her respiratory status, diagnostic bronchoscopy was abandoned. However, the patient was coughing up blood-tinged sputum which was sent for cytology (Figure 2) confirming a diagnosis of non-small cell lung cancer favoring adenocarcinoma. Immunostains performed on sections of the cell block showed malignant cells positive for CK7 and TTF1 and negative for P40 supporting the diagnosis of adenocarcinoma of lung.
This case emphasizes the importance of utilizing noninvasive testing like sputum cytology in patients with severe morbidity to help uncover underlying diagnoses. Studies and medical case reports highlighted the significance of sputum analysis in diagnosing lung cancer (1,2). Challenges posed by this case underscore the importance of considering alternative noninvasive measures to aid in making accurate diagnosis and help patient's and family understanding the underlying etiology of her persistent pneumonia )overall prognosis.
Abdulmonam Ali MD
Pulmonary & Critical Care
SSM Health
Danville, IL USA
References
- Thunnissen FB. Sputum examination for early detection of lung cancer. J Clin Pathol. 2003 Nov;56(11):805-10. [CrossRef] [PubMed]
- Ammanagi AS, Dombale VD, Miskin AT, Dandagi GL, Sangolli SS. Sputum cytology in suspected cases of carcinoma of lung (Sputum cytology a poor man's bronchoscopy!). Lung India. 2012 Jan;29(1):19-23. [CrossRef] [PubMed]
 Post a Comment
Post a Comment