
July 2025 Imaging Case of the Month: A Growing Lung Nodule in a Patient with Heart Disease
Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 36-year-old woman with a history of unspecified anemia, treated with occasional iron infusion, and Hashimoto thyroiditis presented to the Emergency Room with complaints of chest pain, sharp and non-radiating worsening in the supine position and improving with sitting upright and leaning forward, blurred vision, bilateral upper extremity weakness and numbness, and intermittent subjective low-grade fever. These symptoms had been present for about 1 month prior to presentation in the Emergency Room.
The patient’s past medical history was otherwise unremarkable. She is a 20-pack-year smoker with no allergies. Her past surgical history was remarkable only for bilateral breast augmentation, tonsillectomy, and 2 C-sections. Her only medications included a multivitamin and vitamin D3 supplementation.
The patient’s vital signs included a blood pressure of 115/71 mmHg, a pulse rate of 95 / minute, a respiratory rate of 18 / minute and a temperature of 38.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 83.4 kg. The physical examination was largely unremarkable aside from possible symmetric bilateral upper extremity weakness (3/5). Deep tendon reflexes were normal and symmetric bilaterally. In particular, the breath sounds were normal bilaterally.
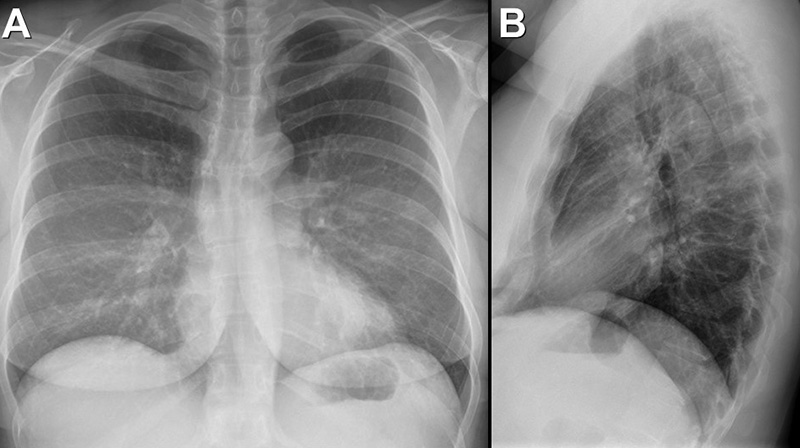
A complete blood count showed a mildly decreased white blood cell count at 3.3 x 109/L (normal, 3.4 – 9.6 x 109/L), with a mildly decreased absolute neutrophil count of 1.4 x 109/L (normal, 1.5 – 7 x 109/L). Her lymphocytes were decreased at 0.71 (normal, 1 – 3.4 x 109/L), but peripheral eosinophilia (30%) was present, and her absolute eosinophil count was elevated at 1.07 x 109/L (normal, 0.0 – 0.4 x 109/L). Her hemoglobin and hematocrit values were mildly decreased at 11.4 gm/dL (normal, 13.5 – 17.5 gm/dL) and 32.3 % (normal, 38.8 – 50%). The platelet count was mildly decreased at 77 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries, including glucose, electrolytes (including calcium), and liver function studies were normal. The urinary drug toxicity screen and pregnancy test were negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. The D-Dimer level was elevated at 2.04 mcg/mL (normal, 0 – 0.49 mcg/mL), and her fibrinogen level was elevated at 654 ng/dL (normal, 200-393 ng/dL). Her troponin-T level was also elevated at 0.124 ng/mL (normal, ≤0.01 ng/mL). Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography shows a normal heart size and normal lung volumes. To view Figure 1 in a separate, enlarged window click here.
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the 2nd of 17 pages)
- The frontal and lateral chest radiograph shows no abnormal findings
- The frontal and lateral chest radiograph shows basal predominant fibrotic abnormalities
- The frontal and lateral chest radiograph shows large lung volumes with a cystic appearance
- The frontal and lateral chest radiograph shows an ill-defined opacity projected over the left base
- The frontal and lateral chest radiograph shows abnormal mediastinal contours
 Post a Comment
Post a Comment


{kind=link}
{kind=link}
{kind=link}
{kind=link}