
Figure 1. Photograph of patient taken ~5 years post double-ling transplant demonstrating multiple cutaneous neurofibromas and an old tracheostomy scar. To view Figure 1 in a separate, enlarged window click here.
{kind=link}

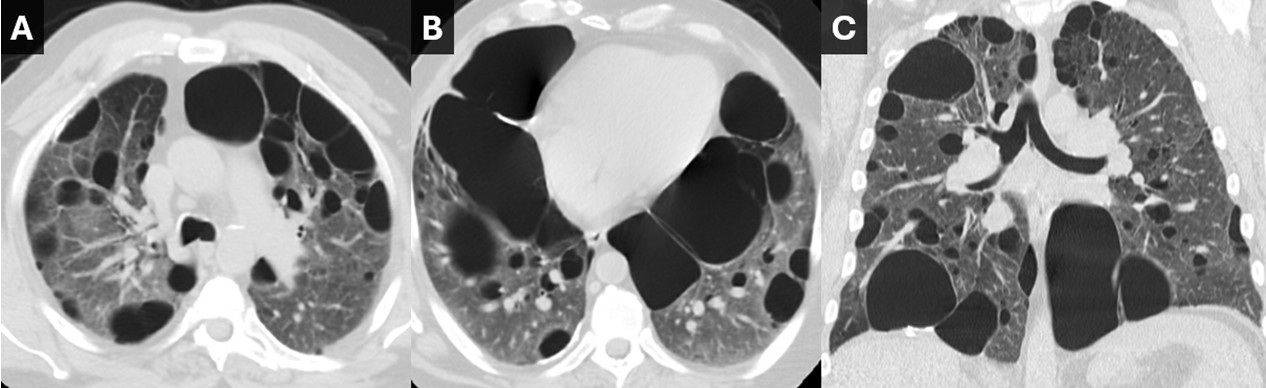
Figure 2. Noncontrast chest CT obtained prior to double lung transplant. Axial images from the upper (A) and lower (B) lungs as well as a coronal (C) reconstruction demonstrate multiple scattered pulmonary cysts, some being very large. There are intervening areas of pulmonary ground glass, perhaps related to atelectasis. To view Figure 2 in a separate, enlarged window click here.
{kind=link}

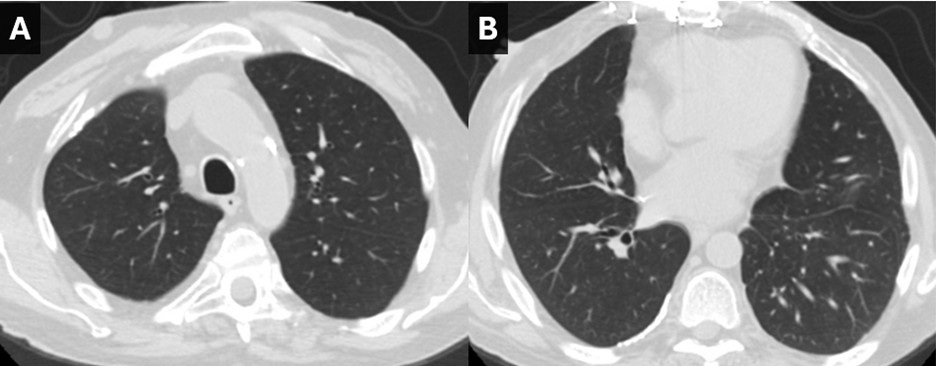
Figure 3. Noncontrast chest CT obtained 5 years after double lung transplant. Axial images from the upper (A) and lower (B) lungs are normal-appearing. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 61-year-old man with a history of neurofibromatosis type 1 (NF1) and NF1-associated cystic lung disease presented for a routine follow-up visit 5 years post-bilateral lung transplantation. The patient’s physical examination revealed multiple cutaneous neurofibromas, consistent with his diagnosis of NF1 (Figure 1). Additionally, he had a prior tracheostomy scar; he temporarily required tracheostomy post lung transplant surgery.
Pre-Transplant History:
The patient had progressive chronic hypoxic respiratory failure, requiring home oxygen supplementation at up to 8 L/min. His medical history included a 15-pack-year smoking history, though he quit smoking 16 years prior to his lung transplant. His diagnostic workup prior to transplant consisted of a high-resolution computed tomography (HRCT) of the chest, which revealed diffuse cystic lung disease with intervening ground-glass opacities (Figure 2), an echocardiogram, which demonstrated severe pulmonary hypertension, and pulmonary function tests (PFTs), which showed a combined restrictive and obstructive pattern with severely reduced DLCO at 25%. Given his progressive respiratory failure and severe pulmonary hypertension, the patient was referred for lung transplant evaluation. He underwent a successful bilateral lung transplant, with post-transplant imaging showing excellent graft function (Figure 3). Post-transplant, the patient achieved an excellent clinical outcome. At 5 years post-transplant, he remains active and reports no significant limitations in his daily activities.
Pulmonary manifestations of NF1, though rare, are increasingly recognized and include upper lobe cystic changes, interstitial lung disease (ILD), and pulmonary hypertension [1, 2). The pathophysiology of NF1-associated diffuse lung disease (NF-DLD) is multifactorial and not fully understood, but several mechanisms have been proposed:
- Abnormal Mesenchymal Development: NF1 is caused by mutations in the NF1 gene, which encodes neurofibromin, a tumor suppressor protein that regulates cell growth and differentiation. Loss of neurofibromin leads to dysregulated mesenchymal cell proliferation, contributing to cystic and fibrotic changes in the lung (1,4).
- Mechanical Stress and Cyst Formation: The cystic changes observed in NF-DLD may result from mechanical stress on the lung parenchyma due to abnormal connective tissue development. This stress can lead to alveolar wall destruction and bullae formation, particularly in the upper lobes (2, 5).
- Nerve Growth Factor (NGF) and Fibrosis: Elevated levels of nerve growth factor (NGF) have been reported in NF1 patients. NGF promotes fibroblast proliferation and collagen deposition, creating a profibrotic environment that may contribute to interstitial lung disease and fibrosis (3, 6).
- Vascular Abnormalities and Pulmonary Hypertension: NF1 is associated with vascular dysplasia, which can lead to pulmonary arterial hypertension (PAH). Chronic hypoxemia secondary to parenchymal lung disease further exacerbates pulmonary hypertension, leading to right ventricular dysfunction, as seen in this patient (7, 8).
- Role of Smoking: While smoking is a known risk factor for lung disease, its role in NF-DLD progression remains unclear. In this case, the patient’s limited smoking history may have contributed to disease progression, but the primary driver was likely NF1-related parenchymal and vascular abnormalities (1, 2).
This case highlights the progressive nature of NF-DLD, which can lead to end-stage lung disease and severe pulmonary hypertension. Early recognition and monitoring of pulmonary complications in NF1 patients are critical. Multidisciplinary care, including referral for lung transplant evaluation, is essential for optimizing outcomes in advanced cases.
Abdulmonam Ali, MD
Interventional Pulmonologist
Pulmonary & Critical Care
Good Samaritan Hospital, SSM Health
Mount Vernon, IL USA
References
- Zamora AC, Collard HR, Wolters PJ, Webb WR, King TE. Neurofibromatosis-associated lung disease: a case series and literature review. Eur Respir J. 2007 Jan;29(1):210-4. [CrossRef] [PubMed]
- Oikonomou A, Vadikolias K, Birbilis T, et al. Neurofibromatosis type 1 presenting with diffuse lung disease. Respir Med Case Rep. 2015;16:1-3.
- Fabricant RN, Todaro GJ. Increased serum levels of nerve growth factor in von Recklinghausen's disease. Arch Neurol. 1981 Jul;38(7):401-5. [CrossRef] [PubMed]
- Riccardi VM. Neurofibromatosis: phenotype, natural history, and pathogenesis. Johns Hopkins University Press. 1992.
- Ryu JH, Parambil JG, McGrann PS, Aughenbaugh GL. Lack of evidence for an association between neurofibromatosis and pulmonary fibrosis. Chest. 2005 Oct;128(4):2381-6. [CrossRef] [PubMed]
- Li Y, O’Connell MP, O’Connell MJ, et al. Nerve growth factor promotes fibroblast migration and collagen production in neurofibromatosis 1. J Invest Dermatol. 2011;131(4):857-864.
- Stewart DR, Cogan JD, Kramer MR, Miller WT Jr, Christiansen LE, Pauciulo MW, Messiaen LM, Tu GS, Thompson WH, Pyeritz RE, Ryu JH, Nichols WC, Kodama M, Meyrick BO, Ross DJ. Is pulmonary arterial hypertension in neurofibromatosis type 1 secondary to a plexogenic arteriopathy? Chest. 2007 Sep;132(3):798-808. [CrossRef] [PubMed]
- Montani D, Coulet F, Girerd B, et al. Pulmonary hypertension in patients with neurofibromatosis type I. Medicine (Baltimore). 2011 May;90(3):201-211. [CrossRef] [PubMed]
Cite as: Ali A. June 2025 Medical Image of the Month: Neurofibromatosis-Associated Diffuse Cystic Lung Disease. Southwest J Pulm Crit Care Sleep. 2025;30(6):63-65. doi: https://doi.org/10.13175/swjpccs006-25 PDF