January 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 68-year-old woman with a history of myelodysplastic syndrome associated with transfusion-dependent anemia and thrombocytopenia presented with recent onset left chest pain and fever. The patient had a remote history of total right knee arthroplasty, hypertension, asthma, and schizoaffective disorder. Several months earlier the patient was hospitalized with methicillin-sensitive Staphylococcus aureus infection involving the right knee arthroplasty, associated with bacteremia and a septic right elbow. This infection was treated with incision and drainage of the elbow, antibiotic bead placement about the right knee arthroplasty with an antibiotic-impregnated spacer, and antibiotics (6 weeks intravenous cefazolin followed by chronic doxycycline suppression therapy, the former later switched to nafcillin and rifampin). The patient had been discharged from the hospital with only compression hose for deep venous thrombosis prophylaxis, owing to her episodes of epistaxis in the setting of transfusion-dependent anemia.
Upon presentation, the patient was hypotensive, tachycardic, and hypotensive. Laboratory data showed a white cell count of 3.9 cells x 109 / L, a platelet count of 7000 x 109 / L, and a hemoglobin level of 7 g/dL.
Frontal chest radiography (Figure 1A) was performed (a baseline chest radiograph- Figure 1B- is presented for comparison).
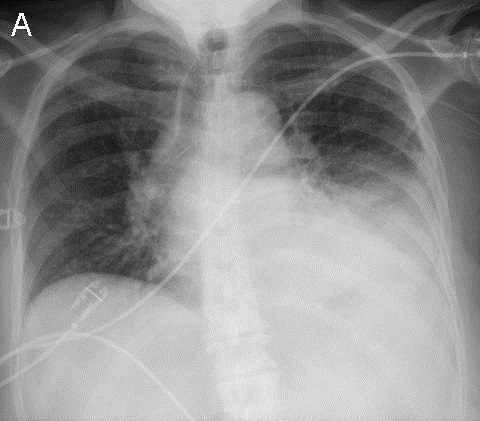
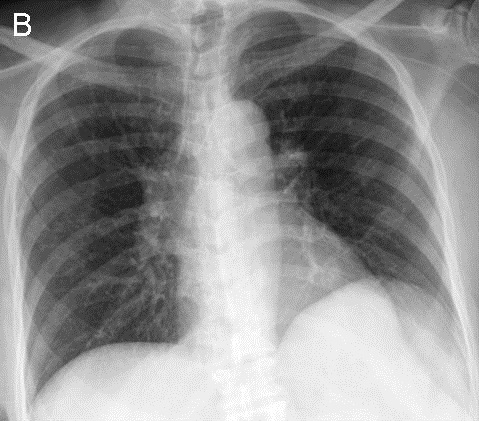
Figure 1. Panel A: Frontal chest radiography Panel B: Frontal chest radiograph obtained 3 months to presentation.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the 2nd of 7 panels)
Reference as: Gotway MB. January 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(1):21-31. doi: http://dx.doi.org/10.13175/swjpcc003-15 PDF
 Post a Comment
Post a Comment