Medical Image of the Week: Post-Traumatic Diaphragmatic Rupture

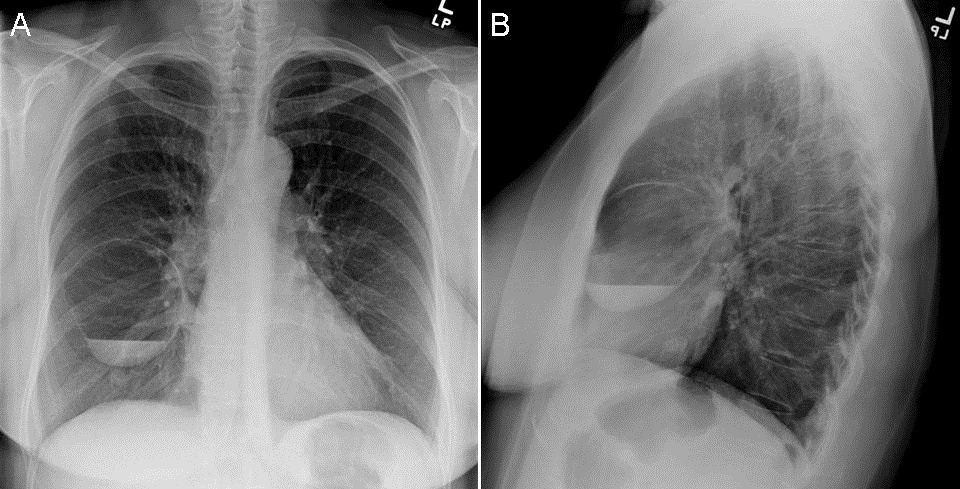
Figure 1. A: Admission portable chest radiograph, demonstrates elevation of the right hemidiaphragm of uncertain chronicity (large arrow, also shown in B and C). B: Study after 20 min, shows a moderate hemothorax (*). Mildly displaced fractures are evident, involving at least the3rd and 5th right ribs (small arrows). C: Follow up exam. A right chest tube (thin arrow in c) has been inserted, and the hemothorax is drained. Immediately after, a CT chest abdomen and pelvis is performed.

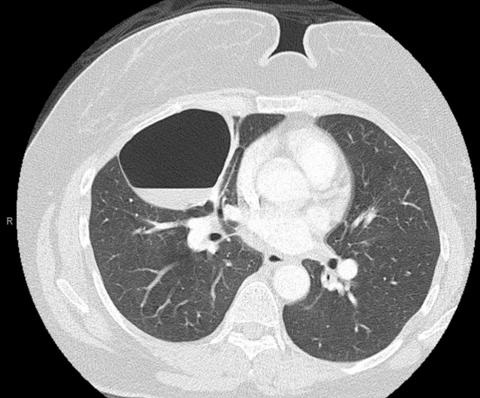
Figure 2. A-C: A large anterolateral diaphragmatic defect is diagnosed, as shown in the coronal images, from anterior to posterior (A-C), with displacement of the liver (L) and loops of bowel (B) into the chest. Note the discontinuity of the diaphragm (arrows in A, B and D). A small liver laceration is noted in the gallbladder bed (arrows in C). D: Image, near the midline, showing atelectasis (A) in the posterior right lung base. Additional injuries (not shown), included, right ribs 2-11 fractures, gallbladder fossa liver, right adrenal hemorrhage, mesenteric root contusion and multiple pelvic fractures.
A 67-year-old woman was admitted after being struck by a vehicle, at high speed. She has a diaphragmatic rupture (Figures 1 and 2).
Diaphragmatic injuries occur in approximately 0.8%–8% of blunt trauma patients, largely from motor vehicle accidents (1). The mechanism of injury includes distortion of the chest wall with resulting shearing forces, or direct frontal impact with acute increased intraabdominal pressure (2).
Rupture of the left diaphragm is more common, presumably due to a protective mechanism by the liver, but also in part due to underdiagnoses (3). Most ruptures are large, posterolateral, between the lumbar and intercostal attachments (4). Associated liver injuries are seen mostly with right diaphragmatic injuries (93 % vs. 24% with left injuries). Multiorgan abdominal injury and pelvic fractures are common (2).
In cases of associated hemothorax, pulmonary laceration/contusion, atelectasis, and phrenic nerve palsy, a diaphragmatic injury, may be masked on chest radiographs. Also, the positive pressure of ventilatory support may delay herniation of abdominal contents through the ruptured diaphragm (5).
Up to 12% to 66% cases of diaphragmatic rupture cases, are missed on chest radiograph. Suggestive findings include elevation of the hemidiaphragm, distortion or obliteration of the outline of the hemidiaphragm, and contralateral shift of the mediastinum (6,7).
On CT visualization of a diaphragmatic defect has most sensitivity and specificity for diaphragmatic injury (73% and 90%) respectively) (8). Intrathoracic herniation of abdominal contents has a sensitivity of 55% and a specificity of 100% (8). The “collar sign”, a waist-like constriction of the herniating hollow viscus at the site of the diaphragmatic tear, is usually seen sagittal and coronal multiplanar reformatted images (2,8). The “dependent viscera sign” (1), consists of bowel or solid organs fallen to a dependent position against the posterior ribs, due to lack of supported by the intact diaphragm. This may be an early sign of diaphragmatic tear on axial images, before visceral herniation is clearly seen on multiplanar reformatted images.
Diana Palacio MD, Veronica Arteaga MD, Berndt Schmidt MD
Department of Medical Imaging
The University of Arizona-Banner Medical Center
Tucson, AZ USA
References
- Bergin D, Ennis R, Keogh C, et al. The "dependent viscera" sign in CT diagnosis of blunt traumatic diaphragmatic rupture. AJR Am J Roentgenol. 2001;177:1137-40. [CrossRef] [PubMed]
- Shanmuganathan K, Killeen K, Mirvis SE, et al. Imaging of diaphragmatic injuries. J Thorac Imaging. 2000;15:104-11. [CrossRef] [PubMed]
- Killeen KL, Mirvis SE, Shanmuganathan K. Helical CT of diaphragmatic rupture caused by blunt trauma. AJR Am J Roentgenol.1999;173:1611-6. [CrossRef] [PubMed]
- Boulanger BR, Milzman DP, Rosati C, et al. A comparison of right and left blunt traumatic diaphragmatic rupture. J Trauma. 1993;35:255-60. [CrossRef] [PubMed]
- Kuhlman JE, Pozniak MA, Collins J, Knisely BL. Radiographic and CT findings of blunt chest trauma: aortic injuries and looking beyond them. RadioGraphics. 1998;18:1085-1106. [CrossRef] [PubMed]
- Iochum S, Ludig T, Walter F, et al. Imaging of Diaphragmatic Injury: A Diagnostic Challenge RadioGraphics 2002; 22:suppl. 1,S103-16. [CrossRef] [PubMed]
- Gelman R, Mirvis SE, Gens D. Diaphragmatic rupture due to blunt trauma: sensitivity of plain chest radiographs. AJR Am J Roentgenol. 1991;156:51-7. [CrossRef] [PubMed]
- Murray JG, Caoili E, Gruden JF, et al. Acute rupture of the diaphragm due to blunt trauma: diagnostic sensitivity and specificity of CT. AJR Am J Roentgenol. 1996;166:10. [CrossRef] [PubMed]
Cite as: Palacio D, Arteaga V, Schmidt B. Medical image of the week: post-trumatic diaphragmatic rupture. Southwest J Pulm Crit Care. 2018;16(3):143-5. doi: https://doi.org/10.13175/swjpcc030-18 PDF
 Post a Comment
Post a Comment