Medical Image of the Week: Fluorescent Urine
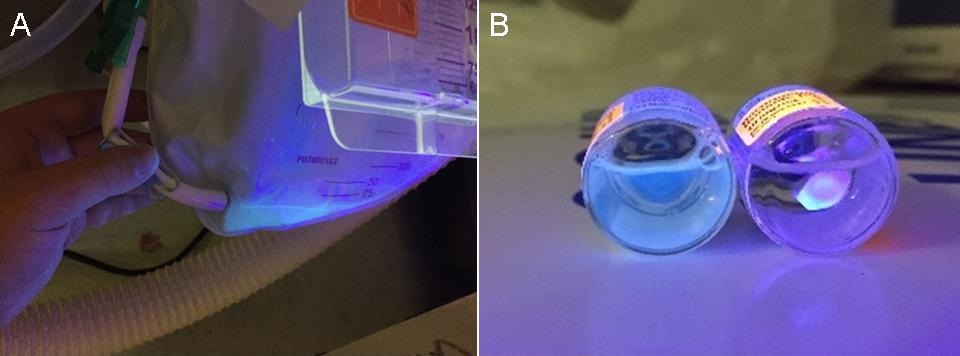
Figure 1. Panel A: urine in Foley catheter collection bag is seen to fluoresce under UV light. Panel B: urine placed in a glass vial (left) relative to saline placed in a glass vial (right) under UV illumination.
A 49-year-old woman presented to the emergency department (ED) via EMS after being found lying on the ground on a hiking path with depressed mental status and confusion. Paramedics found empty bottles of medication surrounding her including quetiapine, clonazepam, and flurazepam, as well as syringes allegedly filled with antifreeze. Because of her severe encephalopathy on presentation, she was intubated shortly after arrival for airway protection. A Foley catheter was placed, and the urine was examined under UV light, revealing fluorescent urine. Ethylene glycol toxicity was suspected given this finding and the history given by EMS; however, initial and then repeat lab studies demonstrated no anion gap, metabolic acidosis, or osmolar gap, and none of these findings developed later during her ICU course. Fomepizole was not administered due to the lack of suggestive lab findings. The patient recovered and was successfully weaned from mechanical ventilation. After extubation, she admitted to taking the medications but explained that she was unable to draw up the antifreeze into the syringe to inject it as planned and did not drink any.
The finding of urine fluorescence can be suggestive of ethylene glycol poisoning, as many antifreeze products contain fluorescein, a fluorescent dye added to assist in identifying coolant leaks. Fluorescein is excreted in the urine when ingested. This fluorescent urine has been suggested as an adjunct test in the diagnosis of ethylene glycol toxicity. In one study, healthy volunteers were given fluorescein doses equivalent to that found in the minimum lethal dose of ethylene glycol (1). Urine fluorescence was found in 75% of these subjects at 1-2 hours post-ingestion and in 48% at 4-6 hours post-ingestion. A study of pediatric patients found a high rate of fluorescence in the urine of normal pediatric volunteers suggesting a poor specificity for the detection of ethylene glycol poisoning (2). Antifreeze products containing propylene glycol, which also contain fluorescein, are now available, and many other substances, including many drugs, nutrients, and food or cosmetic additives have been described to cause urine fluorescence (2). This makes the finding of urine fluorescence under UV light suggestive in the correct clinical setting, but not sufficiently specific to be diagnostic of ethylene glycol ingestion.
Cameron Hypes MD MPH1,2, Phillip Hoverstadt MD MPH2, J. Scott Lowry MD2, Nicholas B. Hurst MD, MS2,3, and F. Mazda Shirazi, MD, PhD2,3
1 Department of Medicine, Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, University of Arizona, Banner University Medical Center; Tucson, AZ
2 Department of Emergency Medicine, University of Arizona, Banner University Medical Center; Tucson, AZ
3 Arizona Poison & Drug Information Center, College of Pharmacy, University of Arizona; Tucson, AZ
References
-
Wallace KL, Suchard JR, Curry SC, Reagan C. Diagnostic use of physicians' detection of urine fluorescence in a simulated ingestion of sodium fluorescein–containing antifreeze. Ann Emerg Med.2001;38(1):49-54. [CrossRef] [PubMed]
-
Casavant MJ, Shah MN, Battels R. Does fluorescent urine indicate antifreeze ingestion by children? Pediatrics. 2001;107(1):113-4. [CrossRef] [PubMed]
Cite as: Hypes C, Hoverstadt P, Lowry JS, Hurst NB, Shirazi FM. Medical image of the week: fluorescent urine. Southwest J Pulm Crit Care. 2015;11(3):103-4. doi: http://dx.doi.org/10.13175/swjpcc083-15 PDF
 Post a Comment
Post a Comment