
Medical Image of the Week: Elemental Mercury Poisoning
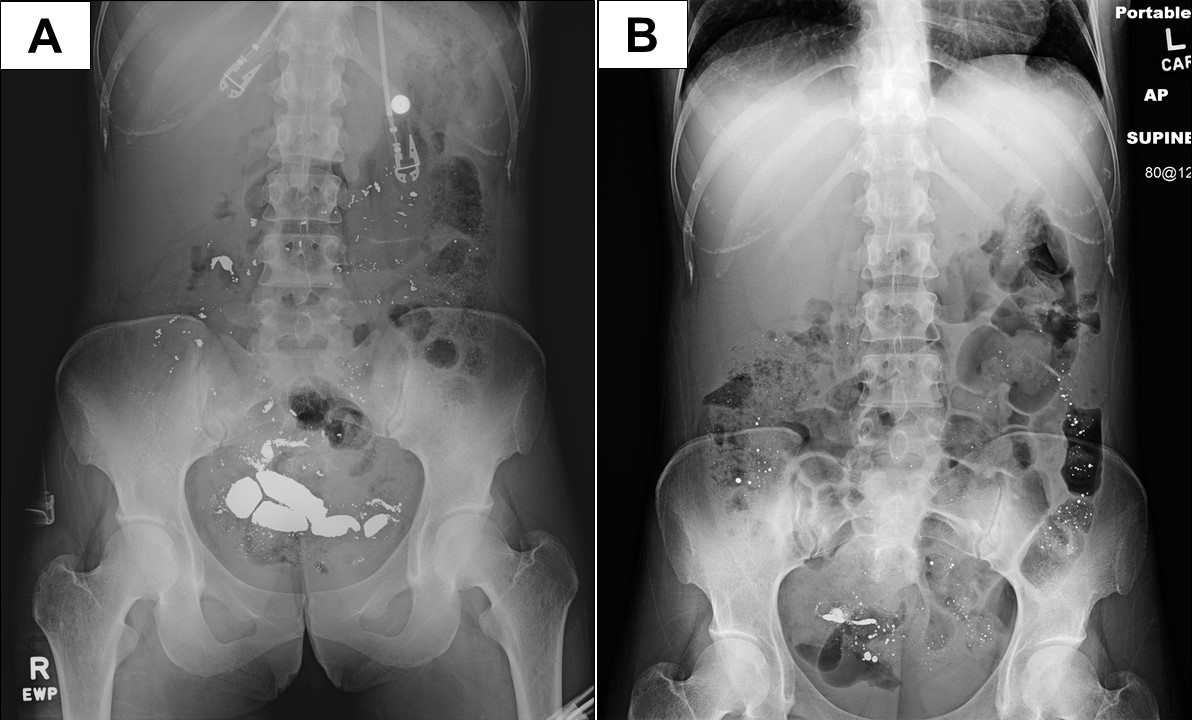
Figure 1. Panel A: Abdominal x-ray showing radiopaque matter. Panel B: Repeat x-ray after colonoscopy.
A 34-year-old woman presented to the Emergency department with abdominal pain after ingestion of an unknown liquid that family felt might be poisonous. The patient had a past history of prior suicide attempts, as well as a history of polysubstance and alcohol abuse. The patient was confused, tangential and a difficult historian. The patient had a heart rate of 72, was normotensive, and had an oxygen saturation of 100% on room air. She was confused and answered questions intermittently. The remainder of her physical examination including her neurological exam was normal. The initial serum chemistry, anion gap, lactate, liver function tests were normal. Urine drug screen was positive for benzodiazepines, for which the patient was prescribed. An abdominal x-ray was performed showing a radiopaque substance in the abdomen (Figure 1A). It was eventually determined she ingested elemental mercury. Blood levels were elevated, and she did eventually have hematochezia. Colonoscopy was performed which removed some of the metallic liquid mercury (Figure 1B).
Mercury in any form is poisonous, with mercury toxicity most commonly affecting the neurologic, gastrointestinal (GI) and renal organ systems (1). Poisoning can result from mercury vapor inhalation, mercury ingestion, mercury injection, and absorption of mercury through the skin.
Elemental mercury is poorly absorbed after ingestion but easily vaporizes at room temperature and is well absorbed (80%) through inhalation. Once absorbed elemental mercury is mostly converted to an inorganic divalent or mercuric form by catalase in the erythrocytes. This inorganic form has similar properties to inorganic mercury (e.g., poor lipid solubility, limited permeability to the blood-brain barrier, and excretion in feces).
Treatment of mercury toxicity consists of removal of the patient from the source of exposure, supportive care, and chelation therapy. Our patient had limited symptoms, and for this reason, chelation therapy was not performed. She made an uneventful recovery after discharge to psychiatry. Her blood levels eventually returned to normal in a few months.
Michel A. Boivin, MD
Pulmonary/Critical Care/Sleep Medicine
Department of Internal Medicine
University of New Mexico
Albuquerque, NM USA
Reference
- Olson DA. Mercury poisoning. Medscape. August 14, 2017. Available at: https://emedicine.medscape.com/article/1175560-overview (accessed 5/22/18).
Cite as: Boivin M. Medical image of the week: Elemental mercury poisoning. Southwest J Pulm Crit Care. 2018;16(5):287-8. doi: https://doi.org/10.13175/swjpcc067-18 PDF
 Post a Comment
Post a Comment
