November 2021 Imaging Case of the Month: Let’s Not Dance the Twist
Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Editor’s Note: Parts of this presentation were used in the June 2020 Pulmonary Case of the Month.
History of Present Illness: An 82-year-old man presented to his physician for general health maintenance as well as a complaint of persistently poor quality sleep and poor appetite with weight loss. The patient had undergone robotic-assisted radical left nephroureterectomy and cystectomy with pelvic lymph node dissection and urinary diversion for left clear cell renal cell carcinoma (staged T2a, grade 2) and transitional cell carcinoma of the bladder (carcinoma in situ at surgery), approximately 9 months earlier. The patient’s bladder malignancy was initially treated with transurethral resection, with histopathology at that procedure showing high-grade papillary urothelial malignancy with lamina propria invasion, but no muscular invasion; this procedure was followed by formal complete resection approximately 3 months later. The patient’s post-operative course was complicated by significant bleeding which required transfusion of 3 units of blood. He had undergone inferior vena caval filter placement prior to surgery when preoperative testing revealed lower extremity deep venous thrombus and pulmonary embolism.
Past Medical History: The patient’s past medical history was remarkable for atrial fibrillation treated with anticoagulation and hypertension. He also had a history of coronary artery disease and myocardial infarction with moderate systolic dysfunction His medical list included warfarin (for his atrial fibrillation), acetaminophen, vitamin supplementation, hydrochlorothiazide, atorvastatin, ramipril, metoprolol, and zolpidem. He denied allergies. The patient was a former smoker, previously smoking 2 packs-per day for 35 years, quitting over 30 years prior to presentation.
His past surgical history was remarkable for laminectomy in addition to the recent urinary surgery. He also had a history of rectal laceration complicating previous prostatectomy for prostate carcinoma (Gleason 3 + 4, T2).
Physical Examination: showed the patient to be afebrile with normal heart and respiratory rates and blood pressure. Her room air oxygen saturation was 99%. The physical examination did not disclose any salient abnormalities.
Initial Laboratory: The patient’s complete blood count and serum chemistries showed largely normal values, with the white blood cell count was normal at 6.7 x 109 /L (normal, 4-10 x 109 /L). His liver function testing and renal function testing parameters were also within normal limits. Echocardiography showed mildly decreased left ventricular systolic function, but this finding was stable. The patient underwent frontal chest radiography (Figure 1A).
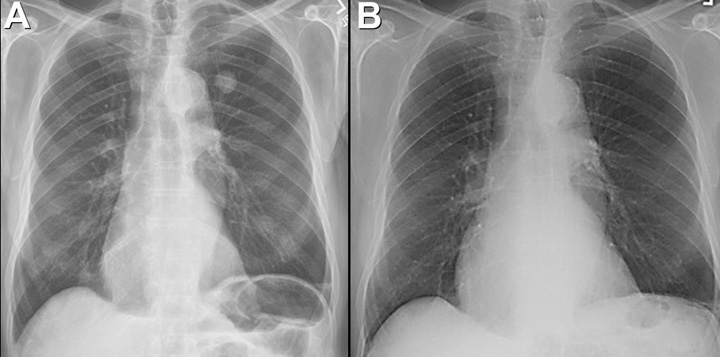
Figure 1. A: Frontal chest radiography. B: Frontal chest radiography performed just over 1 year prior to A shows no specific abnormalities.
Which of the following represents an appropriate interpretation of his frontal chest radiograph? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows no specific abnormalities
- Frontal chest radiograph shows a nodule
- Frontal chest radiography shows bilateral interstitial thickening
- Frontal chest radiography shows bilateral pleural effusions
- Frontal chest radiography shows mediastinal and peribronchial lymph node enlargement
 Post a Comment
Post a Comment