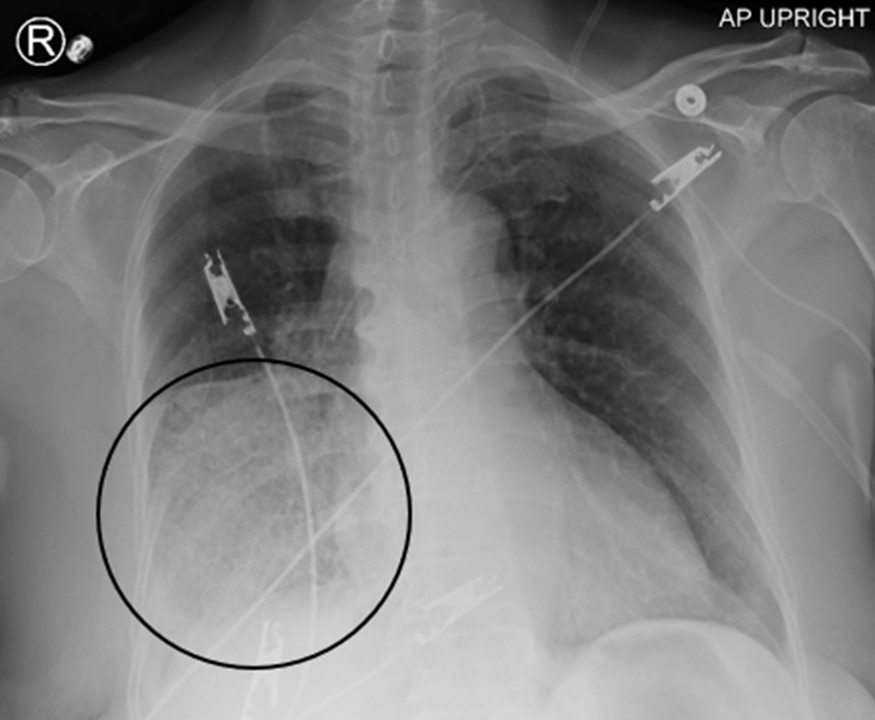
 Figure 1. Portable upright AP chest Xray demonstrating airspace opacities (consolidation and ground glass) in the right lower lobe (circled). Note how the right heart border and medial right hemidiaphragm are not silhouetted out, indicating that the right lower lobe is involved rather than the right middle lobe. Findings originally interpreted as right lower lobe pneumonia. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Portable upright AP chest Xray demonstrating airspace opacities (consolidation and ground glass) in the right lower lobe (circled). Note how the right heart border and medial right hemidiaphragm are not silhouetted out, indicating that the right lower lobe is involved rather than the right middle lobe. Findings originally interpreted as right lower lobe pneumonia. To view Figure 1 in a separate, enlarged window click here.
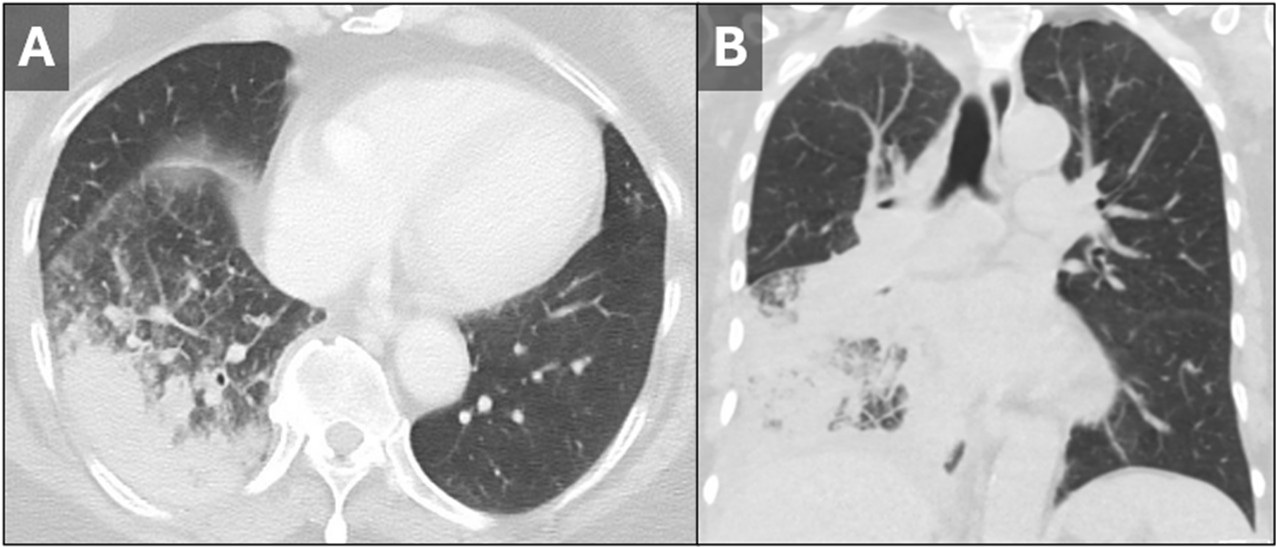
 Figure 2. Axial (A) and coronal (B) lung window reconstructions from a subsequent noncontrast chest CT demonstrating mass-like consolidation in the right lower lobe with adjacent ground glass and septal line thickening. At first glance the findings would be consistent with pneumonia. However, when combined with the patient’s smoking history and the history of RLL consolidation not responding to several courses of antibiotics, malignancy should be excluded. There is also narrowing of the right lower lobe bronchus (B). The septal thickening in this context is concerning for local lymphatic invasion/lymphangitic carcinomatosis. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial (A) and coronal (B) lung window reconstructions from a subsequent noncontrast chest CT demonstrating mass-like consolidation in the right lower lobe with adjacent ground glass and septal line thickening. At first glance the findings would be consistent with pneumonia. However, when combined with the patient’s smoking history and the history of RLL consolidation not responding to several courses of antibiotics, malignancy should be excluded. There is also narrowing of the right lower lobe bronchus (B). The septal thickening in this context is concerning for local lymphatic invasion/lymphangitic carcinomatosis. To view Figure 2 in a separate, enlarged window click here.
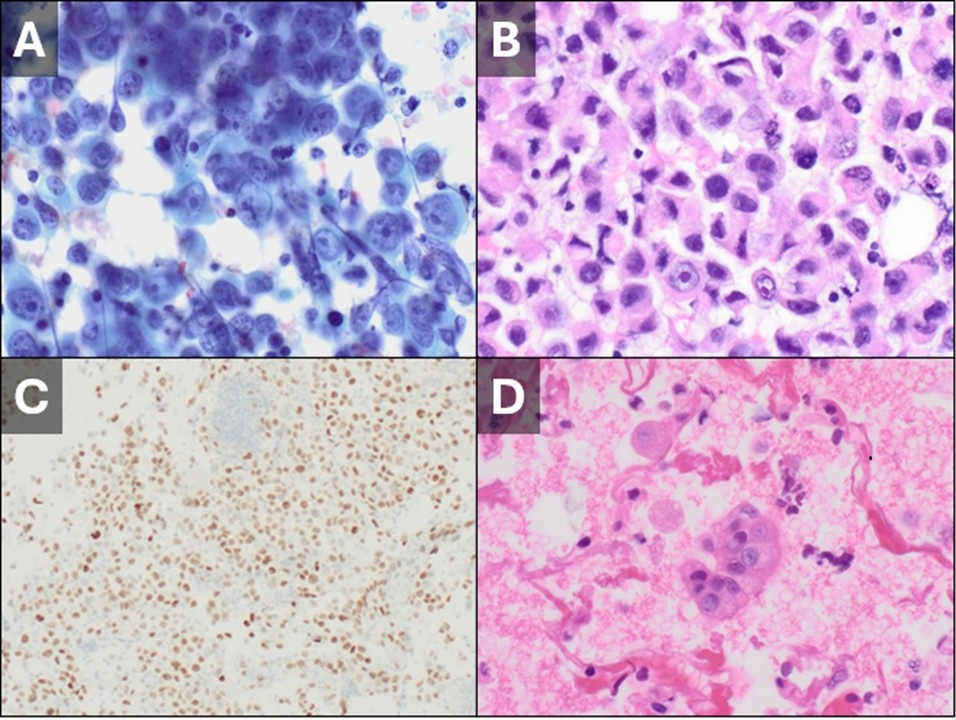
 Figure 3: High-power PAP (A) and H&E (B) stains performed on tissue obtained from fine needle aspiration of right hilar lymph nodes confirmed metastatic involvement of poorly differentiated squamous cell carcinoma. The cells stain positive for TTF-1 (C), consistent with a lung primary. Cultures from bronchoalveolar lavage were negative for infection but showed atypical cells on high-power H&E staining (D). To view Figure 3 in a separate, enlarged window click here.
Figure 3: High-power PAP (A) and H&E (B) stains performed on tissue obtained from fine needle aspiration of right hilar lymph nodes confirmed metastatic involvement of poorly differentiated squamous cell carcinoma. The cells stain positive for TTF-1 (C), consistent with a lung primary. Cultures from bronchoalveolar lavage were negative for infection but showed atypical cells on high-power H&E staining (D). To view Figure 3 in a separate, enlarged window click here.
 Figure 4: An FDG-PET CT performed after discharge demonstrated metabolically hyperactive lymphadenopathy in the right supraclavicular (A), subcarinal, and right mediastinal (B) regions with SUV values as high as 9.5. Mixed ground-glass and solid consolidation in the right lung (C) demonstrated marked metabolic hyperactivity (SUV up to 7.15) consistent with the patient’s history of squamous cell carcinoma. To view Figure 4 in a separate, enlarged window click here.
Figure 4: An FDG-PET CT performed after discharge demonstrated metabolically hyperactive lymphadenopathy in the right supraclavicular (A), subcarinal, and right mediastinal (B) regions with SUV values as high as 9.5. Mixed ground-glass and solid consolidation in the right lung (C) demonstrated marked metabolic hyperactivity (SUV up to 7.15) consistent with the patient’s history of squamous cell carcinoma. To view Figure 4 in a separate, enlarged window click here.
A 63-year-old African American woman with a 30-pack-year smoking history (quit 12 years prior) presented to the emergency room with a persistent cough, throat pain, significant weight loss (15 pounds over 6 months), exertional dyspnea, hoarseness, and fatigue. She denied dysphagia or GERD symptoms and had no other significant medical history. Over four months, she received three courses of antibiotics for presumed lobar pneumonia based on chest X-ray findings. There was no significant clinical improvement, prompting her current visit to the ED. The patient appeared ill and in discomfort. Her vital signs included a blood pressure of 108/73 mmHg (right arm, lying), pulse of 96 bpm, temperature of 99.3 °F (37.4 °C, oral), respiratory rate of 18 breaths/min, and SpO₂ of 91% on room air. Her BMI was 27 kg/m². Physical examination revealed a prominent right supraclavicular lymph node and diminished air entry at the right lung base with a few crackles. There were no signs of edema, no neurological deficits, and no abdominal abnormalities.
A repeat chest X-ray demonstrated persistent right lower lobe (RLL) consolidation (Fig 1). A chest CT revealed RLL mass-like consolidation with a possible underlying mass and interlobular septal thickening, concerning for lymphangitic carcinomatosis (Fig 2). Laboratory results demonstrated hypercalcemia (14.70 mg/dL; normal range [NR]: 8.4–10.2 mg/dL), suppressed PTH (9.8 pg/dL; NR: 15–103 pg/dL), and elevated parathyroid hormone-related peptide (PTHrP) (119 pmol/L; NR: 0.0–3.4 pmol/L), suggestive of malignancy. She received IV broad-spectrum antibiotics for possible post-obstructive pneumonia, but sputum cultures remained negative.
Bronchoscopy with endobronchial ultrasound (EBUS) revealed patent airways with minimal narrowing of the right lower lobe and right middle lobe bronchi due to mucosal swelling. Fine-needle aspiration (FNA) of right mediastinal and hilar lymph nodes, along with bronchoalveolar lavage of the right lower lobe, was performed. Cytology from lymph nodes at stations 4R, 7, and 11Rs confirmed involvement with poorly differentiated squamous cell carcinoma (SCC) (Fig 3A-C). Bronchoalveolar lavage cultures were negative but showed atypical cells (Fig 3D). A repeat chest CT prior to discharge demonstrated persistent RLL consolidation despite 7 days of inpatient IV broad-spectrum antibiotics. The patient tolerated a 6-minute walk test well and did not require home oxygen. An FDG-PET CT performed soon after discharge (Fig 4) revealed hypermetabolism in the RLL consolidation along with hypermetabolic right hilar and mediastinal lymphadenopathy. An enlarged right supraclavicular lymph node with significant hypermetabolism was also noted, likely causing pressure or invasion of the right recurrent laryngeal nerve, explaining her throat pain and hoarseness.
This case illustrates how lung cancer can mimic lobar pneumonia. SCC commonly occurs in smokers, and its symptoms often overlap with acute on chronic bronchitis or pneumonia, especially in early stages. In this patient, the failure of pneumonia-like symptoms to improve with antibiotics and steroids, combined with weight loss, constitutional symptoms, and elevated PTHrP, were red flags prompting further workup (1,2). Persistent lobar consolidation on imaging, despite treatment, was a key indicator of malignancy (3). An invasive diagnostic approach, including bronchoscopy with EBUS, was crucial for confirmation. Elevated PTHrP levels are often associated with paraneoplastic syndromes in malignancies such as SCC. The patient’s neck pain and hoarseness were likely due to the enlarged right supraclavicular lymph node exerting pressure on or invading the recurrent laryngeal nerve. This case highlights the diagnostic challenges of lung cancer presenting as lobar consolidation mimicking pneumonia. Clinicians should maintain a high index of suspicion for malignancy in patients with risk factors and non-resolving symptoms and unchanging imaging findings. A multidisciplinary approach, including advanced imaging and invasive diagnostic techniques, is essential for timely diagnosis and management. This case is also unique, as few reports describe SCC presenting as lobar consolidation; most cases of lung cancer mimicking pneumonia involve adenocarcinoma presenting as non-resolving peripheral consolidation.
Abdulmonam Ali MD1 and Maha Abdulla MD2
1Pulmonary & Critical Care and 2Pathology
SSM Health
Mount Vernon, Illinois, USA
References
- Blackstone N, El-Aini T. Medical image of the month: mucinous adenocarcinoma of the lung mimicking pneumonia. Southwest J Pulm Crit Care. 2021;22(1):8-10. [CrossRef]
- Chaudhary K, Kaur P, Poudel B, Schroeder K, Khatri V. A Case Report of Squamous Cell Carcinoma Misdiagnosed as Cryptogenic Organizing Pneumonia. Cureus. 2023 Jul 27;15(7):e42574. [CrossRef] [PubMed]
- Lee TJ, Leung JWT, Reddy GP, Gotway MB. Persistent lobar consolidation: diagnostic considerations. Clin Pulm Med. 2006; 13(4):258-61. [CrossRef]

 Figure 1. Portable AP chest Xray (A) demonstrating a metallic density projecting over the right hilum. A follow-up chest Xray obtained after bronchoscopy (B) shows that the item is no longer present. Endoscopic view of the right middle lobe bronchus during bronchoscopy (C) and post-retrieval photograph demonstrate a metallic dental screw. To view Figure 1 in a separate , enlarged window click here.
Figure 1. Portable AP chest Xray (A) demonstrating a metallic density projecting over the right hilum. A follow-up chest Xray obtained after bronchoscopy (B) shows that the item is no longer present. Endoscopic view of the right middle lobe bronchus during bronchoscopy (C) and post-retrieval photograph demonstrate a metallic dental screw. To view Figure 1 in a separate , enlarged window click here. Post a Comment
Post a Comment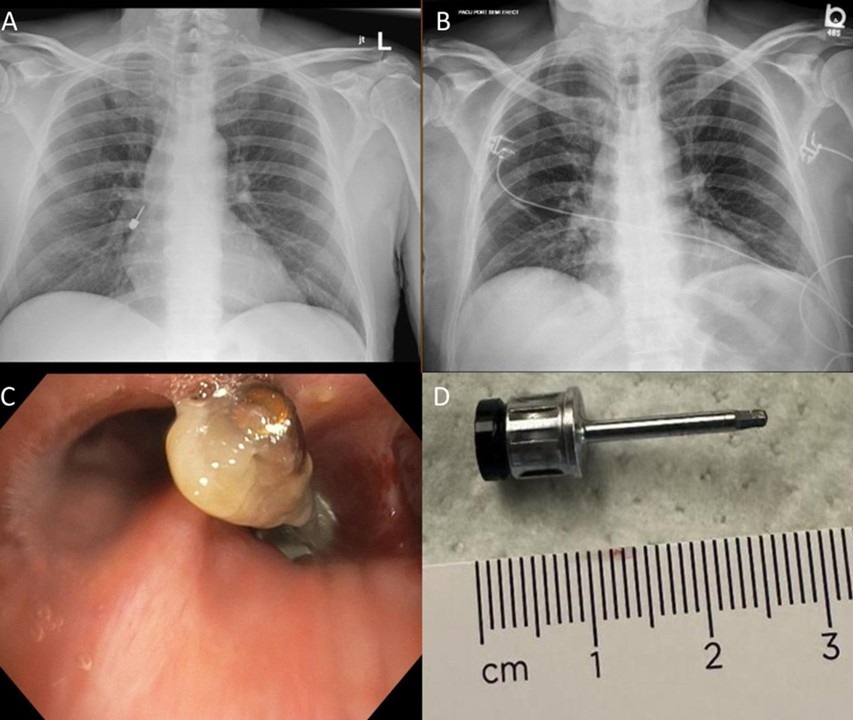{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}