
Correct!
4. Reconsideration of the studies already performed, integrating the history and physical examination.
Further evaluation, including scrotal ultrasound, bone marrow biopsy, AFP and beta-HCG levels, histoplasmosis galactomannan and an interferon-gamma release assay for tuberculosis, were all negative. Critical care, pulmonary, cardiothoracic surgery, and radiology consultants conferred. Upon re-examination of the patient’s history, hospital course and radiological studies, a diagnosis of congenital unilateral pulmonary venous atresia was considered.
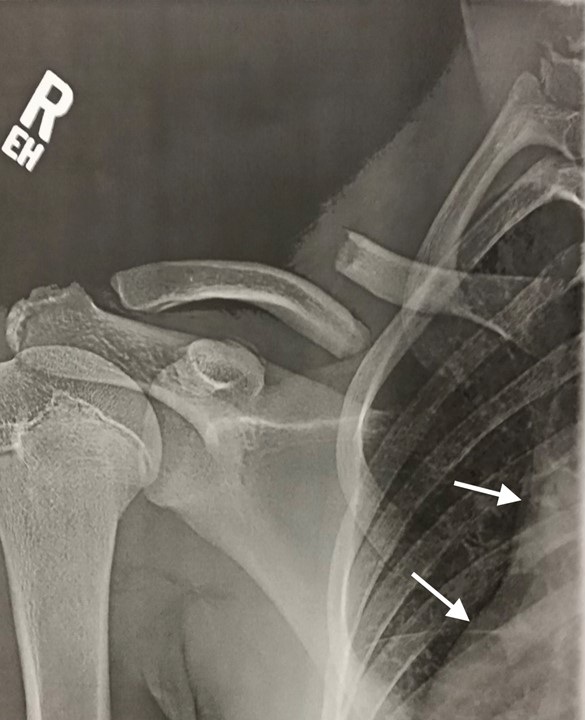
Pursuant to this diagnosis, the radiograph of the patient’s fractured right clavicle taken nine years previously (Figure 3) was obtained, which included a partial view of the right hemithorax, which showed an abnormal right cardiac border consistent with hypoplasia of the right hemithorax and lung, dating back to when the patient was fourteen years old.

Figure 4. Clavicular radiograph from nine years prior to admission showing partial view of abnormal right cardiomediastinal silhouette with mediastinal shift to the right consistent with volume loss of the right hemithorax. To view Figure 4 in a separate, enlarged window click here.
Discussion: Congenital unilateral pulmonary venous atresia (CUPVA) is characterized embryologically by failure of the proximal pulmonary veins to integrate with the left atrium (1,2) and histologically by extensive intimal fibrosis of the pulmonary veins (3). It occurs with equal frequency in the right or left lung, and typically presents early in childhood – about half of the time in association with congenital heart disease (1,4,5). But it can remain unrecognized until adulthood (1,6-11). Clinical manifestations include hemoptysis and recurrent pneumonia. Pulmonary hypertension, pulmonary infarction and variceal bleeding occur less frequently (1,4,7,8,12,13). The radiological features of CUPVA may falsely suggest pulmonary vein obstruction is due to compression or infiltration by malignancy, tuberculosis or fibrosing mediastinitis (1,9)
The diagnosis of CPVA is based on distinctive ipsilateral venous and arterial abnormalities (Figure 4) demonstrable by computerized tomography (CT), magnetic resonance angiography, pulmonary angiography and right heart catheterization (1,4,9,13,14). Imaging findings include: absence of proximal pulmonary veins at their normal site of insertion into the left atrium (1,2), extensive collateralization between the distal pulmonary veins and systemic portal and vena caval systems in the mediastinum (1,15), and interlobular septal thickening consistent with pulmonary venous congestion (1,13,16). The increased resistance of the ipsilateral pulmonary venous system favors redistribution of pulmonary artery flow to the contralateral lung, and increases high-pressure bronchial artery perfusion to the ipsilateral lung. Thus, the ipsilateral pulmonary artery is underdeveloped and the bronchial artery hypertrophies (1,16). This imbalance causes a left-to-right shunt through microvascular channels that connect the bronchial and pulmonary circulatory systems, leading to reversal of flow and increased oxygenation saturation in the ipsilateral pulmonary artery (1,6,16-19). Hypoplasia of the lung itself is likely secondary to reduced pulmonary artery flow, which normally provides >95% of lung perfusion (16).
The clinical findings of CUPVA are relatable to its vascular pathophysiology. Hemoptysis is due to engorgement of the bronchial venous circulation (6,19-21). The confluent mediastinal soft tissue mass actually comprises pulmonary venous collaterals draining into venocaval and portal venous systems (1,4,9,15,17). The later may result in esophageal varices and hematemesis (1,7). Pulmonary hypertension is caused by left-to-right shunting between the bronchial and pulmonary arterial systems resulting in chronic volume and pressure overload of the right ventricle (1,12,13). Pulmonary infarction is due to impaired pulmonary arterial perfusion of the lung (4,8). The increased incidence of pneumonia has been related to impaired mucociliary clearance, local immunity, and lymphatic drainage of the hypoplastic lung (22).
Our patient had clinical and radiographic evidence of all the preceding anatomical and pathophysiological aspects of the disease.
The pathophysiology of CUPVA is illustrated in Figure 5.

Figure 5.Proposed pathophysiology of CUPVA. V1: Atresia of proximal pulmonary vein insertion into the left atrium, V2: mediastinal pulmonary-to-systemic venous collaterals forming a soft-tissue-density mass, V3: esophageal venous engorgement leading to variceal bleeding, V4: engorged bronchial veins resulting in hemoptysis, A1: hypoplasia of pulmonary artery and ipsilateral lung, A2: hyperplastic bronchial artery, A3: left-to-right shunting through shared bronchial-pulmonary arterial microvasculature, A4: reversal of flow in ipsilateral pulmonary artery leading to pulmonary hypertension. To view Figure 5 in a separate, enlarged window click here .
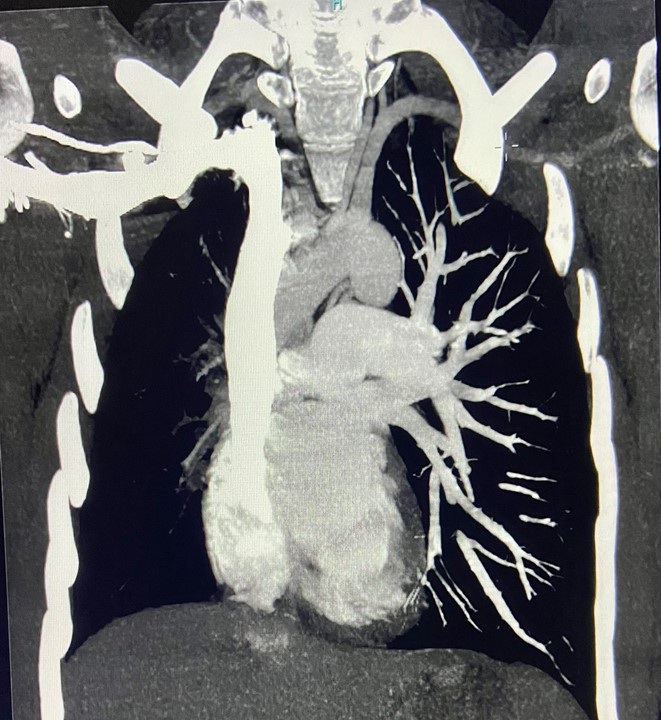
CUPVA may present in adulthood with findings that mimic a primary infiltrative mediastinal process causing external compression of vascular structures. It should be suspected in such patients when initial radiographic findings demonstrate hemithoracic volume loss in the absence of bronchial obstruction (1). Lung scintigraphy – not performed in our case – typically shows absent perfusion of the affected lung (1,15). But the highly asymmetrical pulmonary arterial perfusion characteristic of CUPVA was well demonstrated on the maximum intensity protocol (MIP) image from our patient’s original CTA (Figure 5). Although right heart catheterization with pulmonary arterial wedge angiography was once considered necessary for definitive diagnosis (14,13,23), it has recently been accepted that clinical and CT findings can be virtually pathognomonic (1,4,10,24), as in our case (Figure 6).

Figure 6. Coronal MIP image from the patient’s original CTA, demonstrating highly asymmetric pulmonary artery perfusion favoring the left lung. To view Figure 6 in a separate, enlarged window click here.
Attempts to biopsy the mediastinal mass in CUPVA represent an unnecessary diagnostic misdirection (15,25), with significant bleeding risk.
Although pulmonary infarction has been previously described in CUPVA (4,8), we believe we are the first to report it as a specific complication of bronchial artery embolization in a patient with CUPVA. We believe that abnormal dependence of the affected lung on bronchial artery perfusion likely predisposes to this complication.
Pneumonectomy may benefit patients with CUPVA, eliminating the source of hemoptysis and pneumonia, ameliorating incipient pulmonary hypertension by excising the bronchial-to-pulmonary arterial shunt, and eliminating dead space contributing to exercise intolerance. (13,14). Our patient was transferred to a university-affiliated pulmonary vascular service for further workup and to determine his candidacy for pneumonectomy.
References
{kind=link}
{kind=link}
{kind=link}