
Correct!
All the above.
The patient was admitted and our pulmonary service consulted. He was born in Washington State, moved to Arizona 3 years ago and had not lived elsewhere. He had no prior history of hemoptysis or pneumonia, and had no known exposure to tuberculosis. He worked in a tobacco shop, smoked cigars and vaped THC. He drove to and back from Austin, Texas three weeks prior to admission. His hobbies included hiking and tennis and he had not perceived exercise intolerance. A secondary focused physical examination revealed no lymphadenopathy, splenomegaly or testicular masses. No skin lesions were noted except for a scar over his right clavicle referable to fixation of a clavicular fracture nine years previously.
An echocardiogram showed normal left ventricular size and systolic function with an ejection fraction of 65%. The right ventricle was upper normal size, with normal systolic function. There was trace tricuspid regurgitation, estimated right ventricular systolic pressure was 43 mmHg and mean right atrial pressure was 8 mmHg. A cardiothoracic surgery consultant concluded that mediastinoscopic biopsy of the hypervascular hilar mass was contraindicated due to risk of bleeding. The patient was treated with inhaled and intravenous tranexamic acid, dextromethorphan cough syrup, hydrocodone/homatropine and nebulized lidocaine.
On the second hospital day the patient was intubated for an EBUS-guided transbronchial lymph node aspirate. Bronchoscopy revealed mild luminal narrowing and mucosal thickening of the right mainstem, upper, middle, and lower lobe bronchi with some old blood, but no endobronchial lesions were noted. Ultrasound revealed highly vascular lymphadenopathy at stations 7, 10R and 11R. A large volume aspirate was obtained with a 19-gauge needle from a 2-3cm node in station 10R. Significant bleeding occurred at the biopsy site in the right mainstem bronchus requiring treatment with iced saline lavage, injection of 10cc of 1/10,000 epinephrine and intravenous administration of tranexamic acid. The bleeding was finally controlled but the patient remained intubated on propofol after the procedure. A CT abdomen pelvis was noncontributory, showing no extrathoracic lymphadenopathy, no splenomegaly and no evidence of malignancy, although esophageal varices were noted.
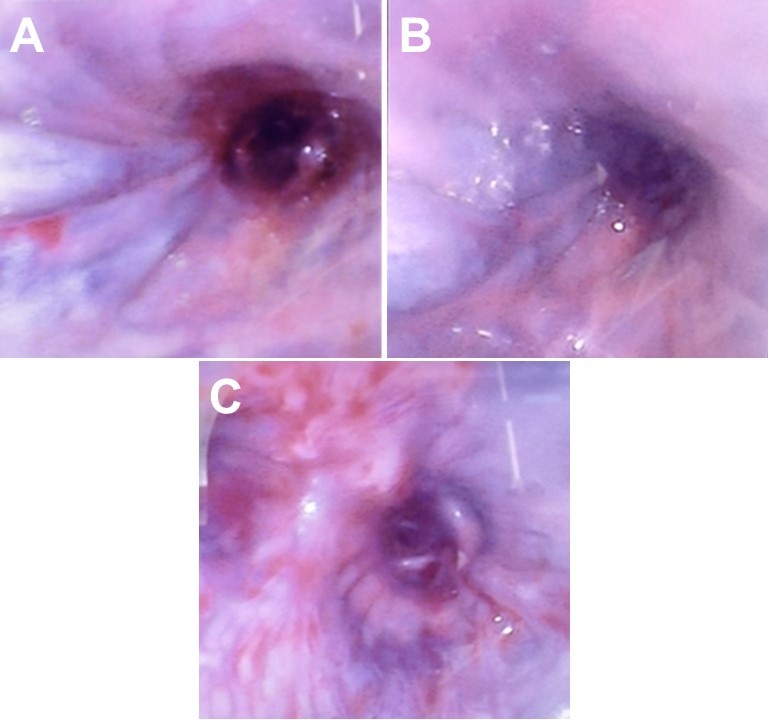
The patient remained intubated, and bronchoscopy was performed daily during the third through fifth hospital days (Figure 3).


Figure 3. Left: (A) & (B) Bronchoscopic views of bronchus intermedius showing dilated submucosal veins extending throughout the length of the airway. (C) Bronchoscopic view of the right lower lobe bronchus showing mucosal hypervascularity due to collateral circulation. To view figure 3A-C in a separate, enlarged window click here. Right: video of bronchsocopy.
Bulging engorged mucosal bronchial veins were noted in the right mainstem bronchus and bronchus intermedius, consistent with bronchial varices. Fresh bleeding was observed originating in the right upper and later from the right lower lobe. Bronchial artery embolization was performed twice before hemoptysis ceased. Cytology and flow cytometry on the EBUS FNA showed only mature lymphocytes, polyclonal B cells and a few epithelial cells. Quantitative culture of the BAL specimen grew only normal flora. Fungal and Legionella cultures showed no growth. Cytological examination of bronchial lavage fluid revealed no malignant cells or coccidioidomycosis spherules. A Nocardia stain and AFB smear were negative. Coccidioidomycosis acute and convalescent phase serologies were negative. Rheumatologic serologies including ANA, RF and ANCA were negative.
The patient spiked a fever to 101.4⁰ on the fifth hospital day. Bronchoscopy revealed purulent appearing secretions obstructing the bronchus intermedius, which were cleared. Empiric piperacillin/tazobactam and vancomycin were administered. Bronchial washings grew methicillin-sensitive Staphylococcus aureus (MSSA) but were again negative for AFB, Nocardia, Legionella, fungi, malignant cells or Coccidioides spherules.
Over the three days, the patient became progressively hypotensive requiring phenylephrine infusion with worsening oxygenation status requiring 100% inspired oxygen. Repeat chest CT angiography showed severe bilateral infiltrates, right side worse than left, consistent with pneumonia. The right lung enhanced significantly less than the left, suggesting pulmonary infarction. The radiologist noted “unchanged bulky mediastinal and right hilar lymphadenopathy with complete encasement of the right mainstem bronchus and complete occlusion of the right superior and inferior pulmonary veins.”
Which of the following are false regarding methicillin-sensitive S. aureus pneumonia? (Click on the correct answer to be directed to the fourth of five pages)
{kind=link}