
Correct!
5. All of the above
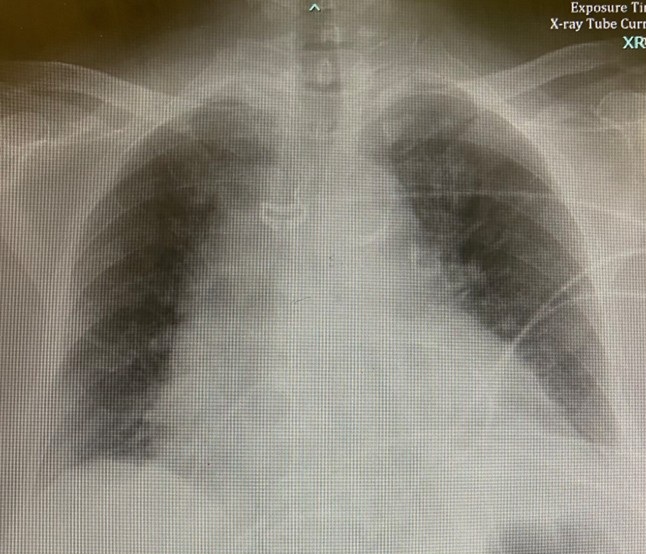
Her initial laboratory evaluation showed WBCC 25.9 109/L, Hg 12.9 g/dL, Na 127 mEq/L, K 4.0 mEq/L, Cl 96 mEq/L, CO2 19 mEq/L, BUN 15 mg/dL, creatinine 0.5 mg/dL, albumin 2.4 mg/dL, ALT 20 U/L, cortisol 62 ug/dL, procalcitonin 33 ng/mL, lactate 3.6 mmol/L, high-sensitivity troponin 261 ng/L, and BNP 307 pg/mL. A chest x-ray was interpreted as showing cardiomegaly and “reticular prominence” of the lung fields bilaterally – both findings new since the chest radiograph performed in the ER two days previously (Figure 3).

Figure 3. CXR on day of admission, two days after the CXR performed in the ER and shown in figure 1. To view Figure 3 in a separate, enlarged window click here.
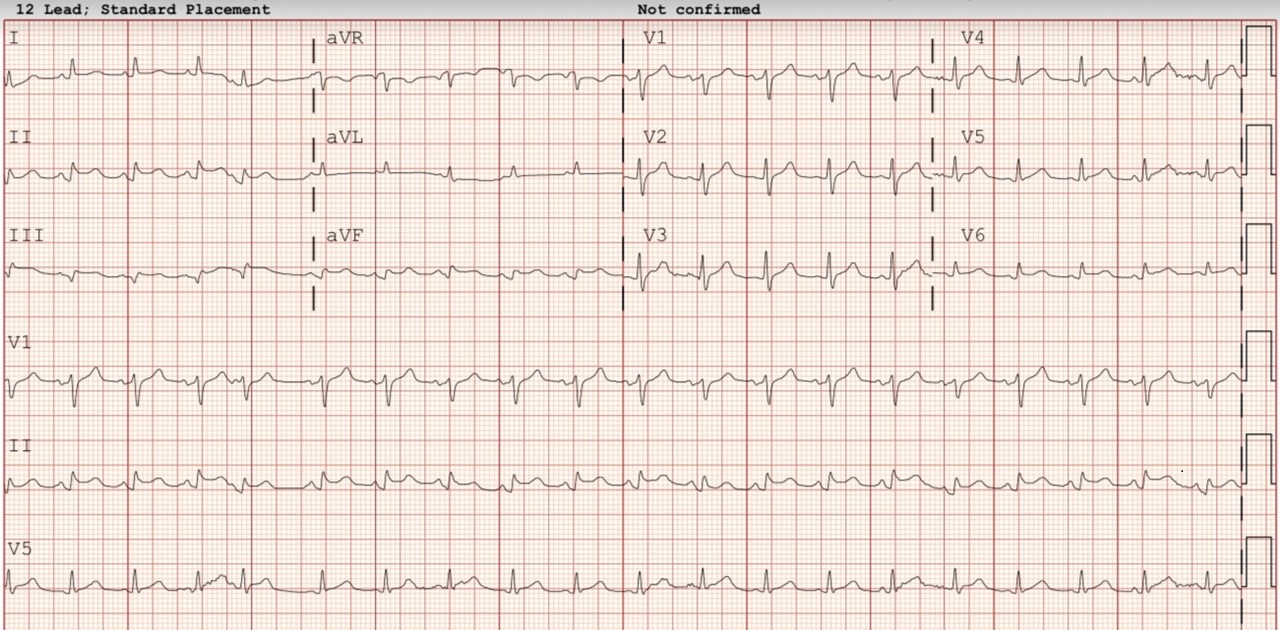
An electrocardiogram (EKG) demonstrated low voltage, ST-elevation and PR depression (Figure 4).

Figure 4. Admission EKG. To view Figure 4 in a separate, enlarged window click here.
Presumptive diagnoses of acute Covid infection, acute coronary syndrome and steroid-induced leukocytosis were made. One liter of normal saline was administered. Blood cultures were drawn. A heparin infusion was started for presumed acute coronary syndrome. At 0300 of the second hospital day (fourteen hours after admission), the family voiced their concern that the patient’s mental status was declining. A repeat lactate was 4.5 mmol/L and a second liter of NS was administered. At 0500, the microbiology laboratory reported that both blood cultures drawn on admission were positive for Gram positive cocci in pairs and clusters, and vancomycin was administered intravenously. At 0700, the patient became diaphoretic and developed respiratory distress. She was afebrile with blood pressure 105/79 mmHg, heart rate 118, and respiratory rate 18 bpm. Her breath sounds were described as coarse, the Glascow coma scale score was eight and her limbs were cool with delayed capillary refill. A repeat lactate rose to 5.2 mmol/L. Sixty-percent FiO2 oxygen was administered by BiPAP and a levophed infusion started. The patient had a bloody bowel movement and the heparin infusion was discontinued. At 0800, the microbiology lab reported that blood cultures were positive for S. aureus DNA and mecA gene by molecular probes.
The patient’s blood pressure progressively fell despite another fluid bolus and increasing doses of norepinephrine infusion.
Which of the following is(are) most likely to account for her progressive clinical decline? (click on the correct answer to be directed to the second of six pages)
{kind=link}
{kind=link}