
Correct!
4. 1 and 3
An echocardiogram was emergently performed, which showed a large pericardial effusion with diastolic impingement of right ventricular filling consistent with cardiac tamponade (Figure 5).

Figure 5. Parasternal short axis view from the echocardiogram showing a large pericardial effusion with diastolic impingement of right ventricular filling consistent with cardiac tamponade. To view Figure 5 in a separate, enlarged window click here .
Before the study concluded, the patient’s blood pressure fell to 60/43 mmHg and heart rate rose to 135 bpm. She appeared agonal. There would appear to be no time for a cardiology or surgical consult. Pericardiocentesis was performed under echocardiographic guidance (Figure 6).

Figure 6. Pericardiocentesis using Seldinger technique under echocardiographic guidance. The guidewire can be seen in the pericardium. To view Figure 6 in a separate, enlarged window click here.
Three hundred mL of grossly purulent pericardial fluid was aspirated, and the patient’s blood pressure rapidly improved. A pigtail drain was placed in the pericardial space. Laboratory analysis of the pericardial fluid revealed 45,000 WBC, 95% neutrophils and Gram stain demonstrated many Gram positive cocci in clusters.
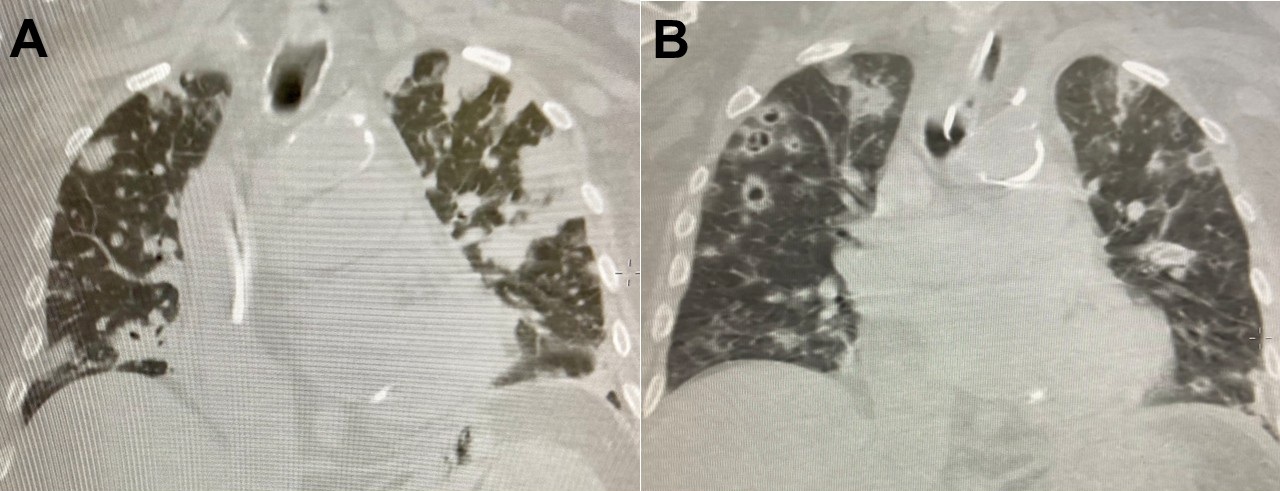
On the third day, the patient’s hypotension and encephalopathy resolved, but her hypoxia worsened, requiring 80% FiO2 by high-low nasal canula. A CXR showed the pericardial drain in good position and new patchy bilateral infiltrates. MRSA grew from the pericardial fluid culture. On the fourth hospital day, a repeat CT chest showed dramatic progression of bilateral multinodular pulmonary infiltrates, consistent with cavitating pneumonia without significant pleural effusion (Figure 7).

Figure 7. Lung CT findings on the fourth (A) and ninth (B) hospital days. To view Figure 7 in a separate, enlarged window click here.
An echocardiogram showed no reaccumulation of pericardial effusion and no vegetations. On the sixth hospital day, the patient experienced progressive respiratory failure and was intubated. Bronchoalveolar lavage was performed revealing grossly purulent sputum which grew MRSA, despite the patient having received six days of vancomycin. A transesophageal echocardiogram (TEE) showed no reaccumulation of pericardial effusion and no evidence of endocarditis. Blood cultures from the first, second, third, fourth and sixth hospital days all eventually grew MRSA.
Which of the following are true regarding vancomycin treatment failure in patients with MRSA infection? (click on the correct answer to be directed to the fourth of six pages)
{kind=link}
{kind=link}
{kind=link}