
Correct!
3. Bronchoscopy
The diagnosis of possible left lower lobe broncholithiasis should be confirmed with bronchoscopy. Pulmonary medicine was consulted, and bronchoscopy (Figure 8) was performed.

Figure 8. Bronchoscopy showing left lower lobe broncholith encroaching upon the airway lumen. To view Figure 8 in a separate enlarged window, click here.
Bronchoscopy showed a normal larynx, vocal cords, and trachea. The entire tracheobronchial tree was examined to at least the first subsegmental level, showing normal bronchial mucosa; no endobronchial lesions and no secretions were seen, except in the left lower lobe where a large broncholith was noted eroding into the carina between the superior segment and left lower lobe segmental airways. Some friability noted with suction was noted, but no active bleeding was seen. Bronchoalveolar lavage was performed in the left upper lobe of the lung and sent for cell count, bacterial culture, viral smears and culture, fungal and acid-fast bacilli analysis using the compromised host protocol. 80 mL of fluid were instilled, 40 mL were returned, blood tinged. There were no mucoid plugs in the returned fluid.
The bronchoscopy evaluation returned gram positive bacilli, many white blood cells, and RSV. Azithromycin was begun, on the assumption that the gram-positive bacilli could represent Actinomyces. Ribavirin was initiated. Thoracic surgery was consulted but was reluctant to intervene, citing the lack of hemoptysis, the patient’s immunosuppression, and the fear of possible adhesions and complications from thoracotomy in the context of previous coronary artery bypass grafting surgery. The consulting surgeon advised repeat CT and follow up in 8 months.
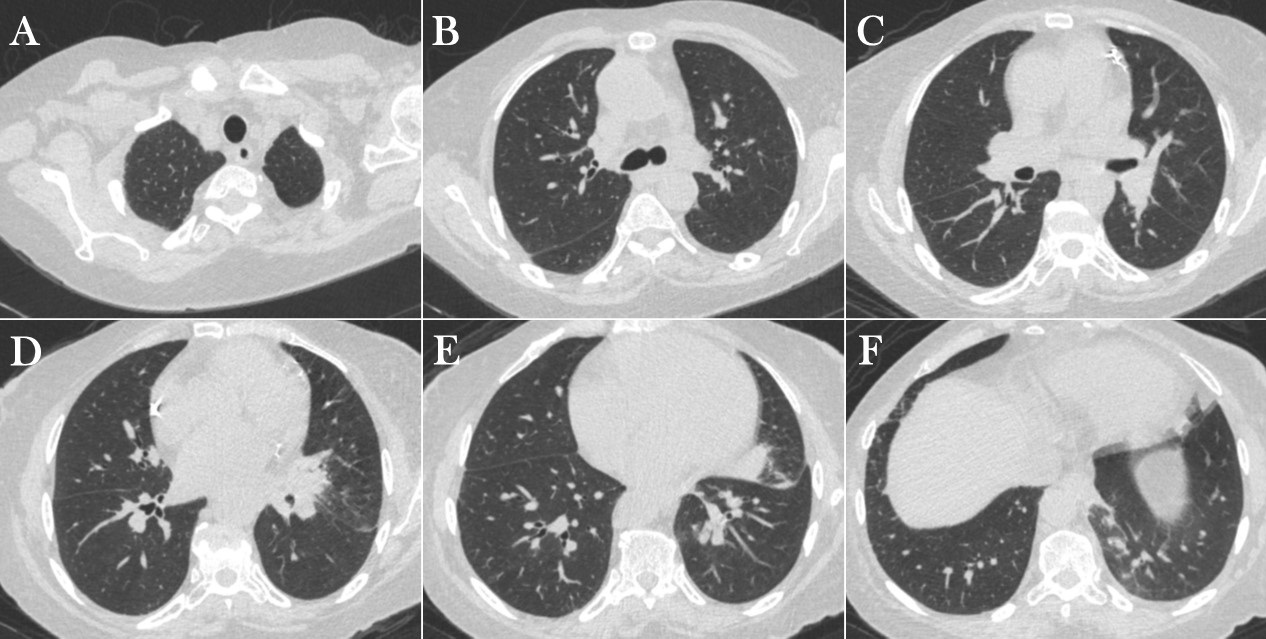
The patient re-presented to the Emergency Room 3 months later again with symptoms of cough and low-grade fever. Repeat unenhanced chest CT (Figure 9) was performed.


Figure 9. Left: Unenhanced chest CT performed 3 months after the diagnosis of broncholithiasis in lung windows. To view Figure 9 in a separate, enlarged window, click here. Right: Video of chest CT in lung windows.
Which of the following represents an appropriate interpretation for this examination? (Click on the correct answer to be directed to the eleventh of 12 pages)
{kind=link}
{kind=link}