CMS Penalizes 758 Hospitals for Safety Incidents
The Centers for Medicare and Medicaid Services (CMS) is penalizing 758 hospitals with higher rates of patient safety incidents, and more than half of those were also fined last year, as reported by Kaiser Health News (1).
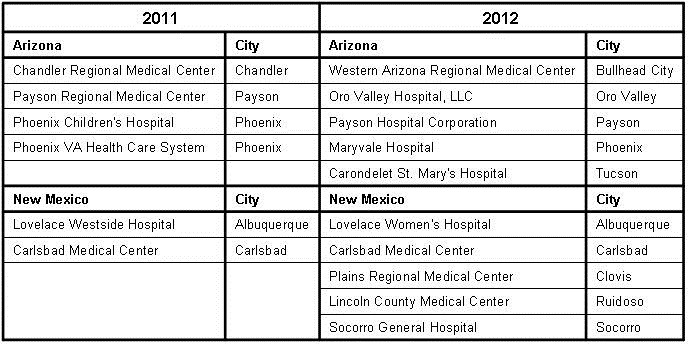
Among the hospitals being financially punished are some well-known institutions, including Yale New Haven Hospital, Medstar Washington Hospital Center in DC, Grady Memorial Hospital, Northwestern Memorial Hospital in Chicago, Indiana University Health, Brigham and Womens Hospital, Tufts Medical Center, University of North Carolina Hospital, the Cleveland Clinic, Hospital of the University of Pennsylvania, Parkland Health and Hospital, and the University of Virginia Medical Center (Complete List of Hospitals Penalized 2016). In the Southwest the list includes Banner University Medical Center in Tucson, Ronald Reagan UCLA Medical Center, Stanford Health Care, Denver Health Medical Center and the University of New Mexico Medical Center (for list of Southwest hospitals see Appendix 1). In total, CMS estimates the penalties will cost hospitals $364 million. Look now if you must, but you might want to read the below before on how to interpret the data.
The penalties, created by the 2010 health law, are the toughest sanctions CMS has taken on hospital safety. Patient safety advocates worry the fines are not large enough to alter hospital behavior and that they only examine a small portion of the types of mistakes that take place. On the other hand, hospitals say the penalties are counterproductive and unfairly levied against places that have made progress in safety but have not caught up to most facilities. They are also bothered that the health law requires CMS to punish a quarter of hospitals each year. CMS plans to add more types of conditions in future years.
I would like to raise two additional concerns. First, is the data accurate? The data is self-reported by the hospitals and previously the accuracy of these self reports has been questioned (2). Are some hospitals being punished for accurately reporting data while others rewarded for lying? I doubt that CMS will be looking too closely since bad data would invalidate their claims that they are improving hospital safety. It seems unlikely that punishing half the Nation's hospitals will do much except encouraging more suspect data.
Second, does the data mean anything? Please do not misconstrue or twist the truth that I am advocating against patient safety. What I am advocating for is meaningful measures. Previous research has suggested that the measures chosen by CMS have no correlation or even a negative correlation with patient outcomes (3,4). In other words, doing well on a safety measure was associated with either no improvement or a negative outcome, in some cases even death. How can this be? Let me draw an analogy of hospital admissions. About 1% of the 35 million or so patients admitted to hospitals in the US die. The death rate is much lower in the population not admitted to the hospital. According to CMS' logic, if we were to reduce admissions by 5% or 1.75 million, 17,500 lives (1% of 1.75 million) would be saved. This is, of course, absurd.
Looking at hospital acquired infections which make up much of CMS' data, CMS' logic appears similar. For example, insertion of urinary catheters, large bore central lines or endotracheal intubation in sick patients is common. The downside is some will develop urinary, line or lung infections as a complication of these insertions. Many of these sick patients will die and many will have line infections. The data is usually reported by saying hospital-acquired infections have decreased saving 50,000 lives and saved $12 billion in care costs (5). However, the truth is that hospital-acquired infections are often either not the cause of death or the final event in a disease process that caused the patient to be admitted to the hospital in the first place. If 50,000 lives are saved that should be reflected in the hospital death rates or a savings on insurance premiums. Neither has been shown to my knowledge.
So look at the data if you must but look with a skeptical eye. Until CMS convincingly demonstrates that the data is accurate and that their incentives decrease in-hospital complications, mortality and costs-the data is suspect. It could be as simple that the hospitals receiving the penalties are those taking care of sicker patients. What this means is that some hospitals, perhaps the ones that need the money the most, will have 1% less CMS reimbursement, which might make care worse rather than better.
Richard A. Robbins, MD
Editor
SWJPCC
References
- Rau J. Medicare penalizes 758 hospitals for safety incidents, Kaiser Health News. December 10, 2015. Available at: http://khn.org/news/medicare-penalizes-758-hospitals-for-safety-incidents/ (accessed 12/11/15).
- Robbins RA. The Emperor has no clothes: the accuracy of hospital performance data. Southwest J Pulm Crit Care 2012;5:203-5.
- Robbins RA, Gerkin RD. Comparisons between Medicare mortality, morbidity, readmission and complications. Southwest J Pulm Crit Care. 2013;6(6):278-86
- Lee GM, Kleinman K, Soumerai SB, et al. Effect of nonpayment for preventable infections in U.S. hospitals. N Engl J Med. 2012;367(15):1428-37. [CrossRef] [PubMed]
- Department of Health and Human Services. Efforts to improve patient safety result in 1.3 million fewer patient harms, 50,000 lives saved and $12 billion in health spending avoided. December 2, 2014. Available at: http://www.hhs.gov/about/news/2014/12/02/efforts-improve-patient-safety-result-1-3-million-fewer-patient-harms-50000-lives-saved-and-12-billion-in-health-spending-avoided.html (accessed 12/11/15).
Cite as: Robbins RA. CMS penalizes 758 hospitals for safety incidents. Southwest J Pulm Crit Care. 2015;11(6):269-70. doi: http://dx.doi.org/10.13175/swjpcc153-15 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.