
Correct!
1. The right lung mass shows an “incomplete border” sign
The “incomplete border” sign (Figure 3A) is present when a lesion shows a circumscribed margin on one side, and an obscured, or “fading” margin on the other side- this configuration is typical of extraparenchymal lesions, such as those arising from the pleura or chest wall.
The patient underwent unenhanced and enhanced chest CT (Figure 4) for further evaluation of the chest radiographic abnormality.

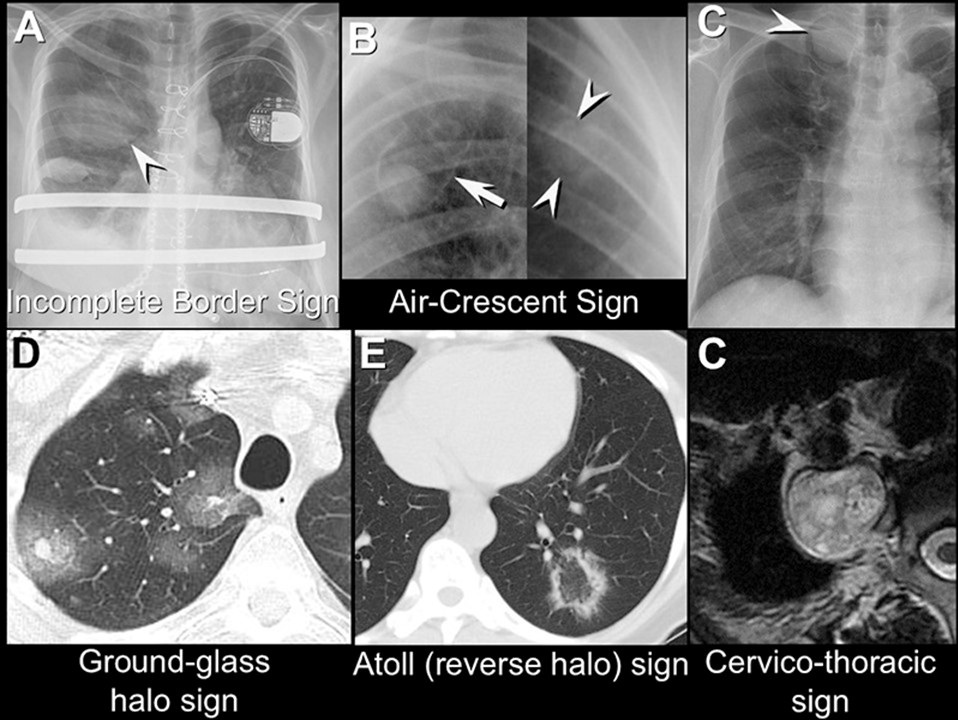
Figure 3. Imaging signs. A: “Incomplete border” sign. Note the circumscribed inferior margin (arrowhead) of the opacity overlying the right upper lobe, with the cranial margin of this opacity “fading” indistinctly. The cause of the finding was multiloculated pleural effusion. B: “Air-crescent” sign. Image on left shows mycetoma- Aspergillus fungal ball complicating a pre-existing cavity (arrow). Image on right shows angioinvasive fungus (Aspergillus) causing a nodule with peripheral lucency (arrowheads) in a patient recovering from profound neutropenia. C: “Cervico-thoracic sign. Note how the lateral margin of the lesion (arrowhead) can be readily seen to the level of the 1st posterior costovertebral junction, consistent with a posterior mediastinal lesion; the abnormality was due to a schwannoma. D: “Ground-glass halo” sign. Note several lung nodules with central, solid foci of opacity surrounded by ground-glass opacity, due to hemorrhagic metastases. E: “Atoll” (aka, “reverse halo” or “reverse ground-glass halo”) sign. Note focal opacity with central ground-glass opacity surrounded by consolidation, due to organizing pneumonia. To view figure 3 in a separate, enlarged window click here.
The “air-crescent” sign reflects a solid lesion within a cavity, which creates a crescent-shaped lucent gas-containing focus between the wall of the cavity and the internal opacity (Figure 3B). The “air-crescent” sign can be seen in patients with pre-existing cavities (mycetoma) or in patients with angioinvasive fungal infections recovering from profound immunosuppression [Figure 3B]. The ‘cervico-thoracic” sign (Figure 3C) describes the appearance of a mediastinal lesion near the thoracic inlet. At the thoracic inlet, the anterior first ribs and clavicle demarcate the anterior aspect of the lung, whereas the posterior lung extends more cranially. Therefore, a lesion in the anterior mediastinum will show a sharply demarcated contour to the level of the first ribs and clavicle,above which such a lesion will enter the neck, thereby losing contact with the lung, resulting in “disappearance” of the abnormal contour. In contrast, a lesion in the posterior mediastinum will maintain contact with the lung to the level of the posterior first rib, and therefore the abnormal contour on the chest radiograph will extend more cranially in the presence of a posterior mediastinal lesion compared with an anterior mediastinal lesion. The “ground-glass halo” sign (Figure 3D) is a CT sign that represents a solid, nodular area of consolidation surrounded by ground-glass opacity, and is typical of a hemorrhagic lesion, often encountered in the setting of invasive fungal infection in severely immunocompromised patients. The “atoll” sign, or “reverse ground-glass halo” sign (Figure 3E), is also an imaging finding seen at CT in which a nodular focus of ground-glass opacity is surrounded by a partial or complete ring of consolidation, is often encountered in patients with organizing pneumonia.Regarding the chest radiograph (Figure 1) and the finding of an “incomplete border” sign, which of the following is correct? (click on the correct answer to be directed to the fourth of 11 pages)
{kind=link}