
Correct!
2. Percutaneous transthoracic needle aspiration and core biopsy
A number of possibilities for obtaining a tissue diagnosis are available, but percutaneous transthoracic biopsy allows both cytologic and histologic sampling (the latter via core biopsy) while still providing the least invasive approach. Video-assisted thoracoscopic surgery certainly could provide a diagnosis. Mediastinoscopy is not appropriate as this procedure cannot access the mass. Bronchoscopy may be able to access the lesion, but the smaller biopsy sizes and the peripheral nature of the lesion make percutaneous transthoracic biopsy preferable. Cryobiopsy provides a larger sample than bronchoscopic biopsy and allows histologic sampling [important in this circumstance given the possibility of a spindle cell neoplasm], but the peripheral nature of the lesion makes this procedure less desirable than percutaneous transthoracic biopsy.
The patient underwent robotic cryobiopsy without complications. The bronchioloalveolar lavage showed only acute inflammation, endobronchial biopsy of mediastinal and peribronchial lymph nodes revealed no abnormality, but the navigational bronchoscopic biopsy of the mass showed a spindle cell neoplasm with tumor cells positive for CD99, CD34 and STAT6, and negative for desmin, SMA, cytokeratin AE 1/3 synaptophysin, CD45 and SOX10. These histopathological features were considered consistent with solitary fibrous tumor of the pleura.
The patient underwent thoracic surgery for resection of the lesion. During the operation a stalk was identified originating from the visceral pleura over the right lower lobe extending into the lesion. Several vascular adhesions connecting the mass to the right upper and lower lobe were encountered, requiring lung wedge resection, but there was no evidence of actual invasion by the mass into the adjacent lung or chest wall and the mass was completely removed (Figure 8).

Figure 8. Gross specimen following surgical resection. To view Figure 8 in a separate, enlarged window click here.
Several additional areas of pleural nodularity were encountered and were resected (Figure 9).

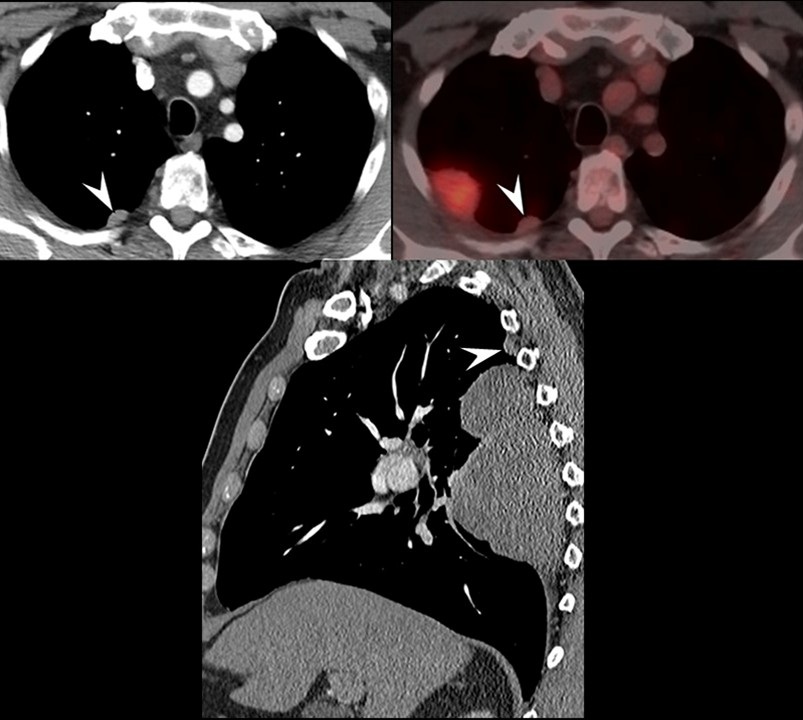
Figure 9. An additional pleural lesion, separate from the dominant mass, is evident (arrowheads). Several such lesions were seen during the operation to resect the dominant lesion. To view figure 9 in a separate, enlarged window click here.
Pathological analysis revealed a lesion measuring 20.2 cm with high-grade de-differentiation, 4 mitoses per 10 high power fields, and 20% of the tumor showing necrosis. A risk assessment model has been validated for solitary fibrous tumor, utilizing scores related to the patient's age, tumor size, mitotic count, and present or absence of tumor necrosis (9). The model for this patient predicts intermediate risk (10% risk of metastasis at 10 years) for his neoplasm.
Diagnosis: Solitary fibrous tumor of the pleura, de-differentiated
References
{kind=link}
{kind=link}