
Correct!
3. Repeat chest radiography
While unenhanced chest CT is not an incorrect answer, there is relatively little in the patient’s clinical history that suggests the need for cross sectional imaging, given that her most recent chest radiograph appeared relatively normal. No objective evidence of active intrathoracic infection is present. The indeterminate results for coccidioidomycosis could represent an indication to proceed with chest CT rather than repeat chest radiography, although follow up for the indeterminate serologies will be required regardless of the chest CT findings. There are no identified risk factors for pulmonary embolism nor is the patient’s presentation overtly suggestive of such. It would be appropriate to consider d-dimer testing, given her non-high risk for acute pulmonary embolism; negative results would allow any consideration for CT pulmonary angiography to be deferred. Neither 18FDG-PET scan nor contrast-enhanced MR have a role for the evaluation of this patient’s complaints, particularly form the emergency room.
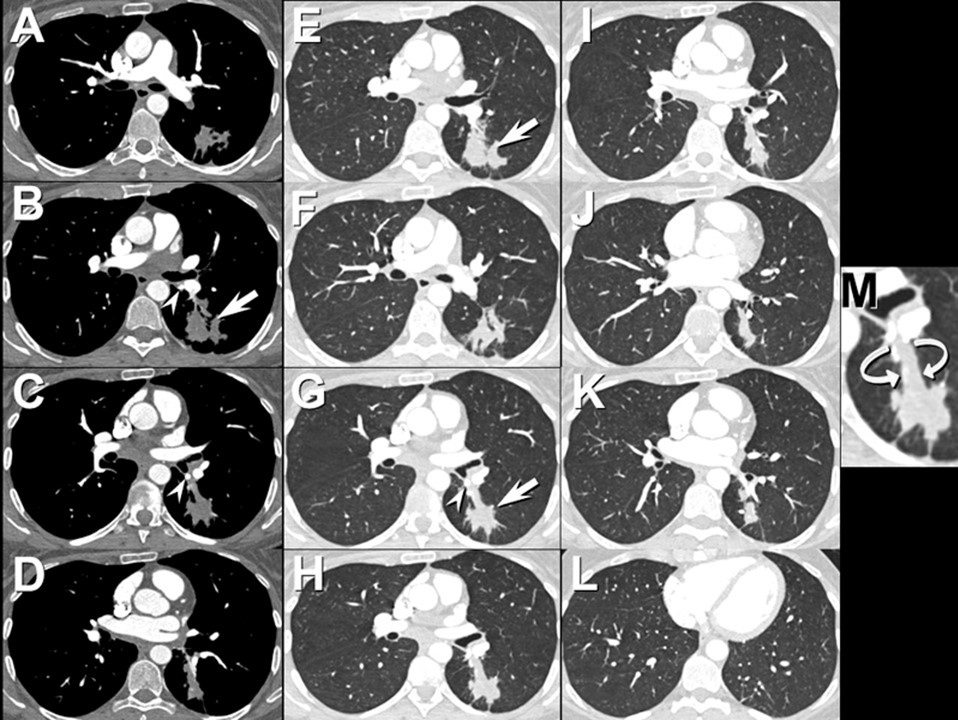
The patient underwent CT pulmonary angiography (Figure 5).

Figure 5. Axial enhanced chest CT performed according to a pulmonary embolism protocol shows superior segment left lower lobe consolidation (arrows) and mild left peribronchial lymph node enlargement. Calcified left peribronchial lymph nodes are present (arrowheads). A patent superior segmental left lower lobe bronchus is not seen; rather a tubular-shaped opacity is present in this location (curved arrows, inset image M) with a focus of calcification at the orifice of the bronchus. Click here to view Figure 5 in an enlarged window.
Which of the following represents an appropriate interpretation for this examination? (Click on the correct answer to be directed to the seventh of 11 pages)
{kind=link}