
Infectious Diseases Telemedicine to the Arizona Department of Corrections During SARS-CoV-2 Pandemic. A Short Report.
Stephen A. Klotz MD, Krystal R. Fimbres, Lawrence D. York PharmD
Division of Infectious Diseases, University of Arizona-Tucson
Tucson, Arizona USA
Abstract
The University of Arizona infectious diseases provides telemedicine clinics to the Arizona Department of Corrections (DOC) and Pima County Jail. Beginning in January 2020 there was a sharp drop in the number of monthly consultations following the public health emergency regarding the SARS-CoV-2 pandemic. Only since ending the emergency have the number of consults risen each month to pre-pandemic numbers. However, the nature of consult requests has changed. In this report we document the change from predominately human immunodeficiency virus (HIV) consults to a broader spectrum of infectious-related issues, most noteworthy being infective endocarditis, osteomyelitis, and chronic hepatitis B and C infection, the majority of cases due to intravenous drug injection. Although the DOC and jail underwent major upheavals intramurally due to the pandemic, medical outcomes with the diseases listed above, were excellent. The telemedicine infectious diseases clinics continued to provide timely, effective care for inmates.
Introduction
A University of Arizona telemedicine clinic for infectious diseases has been held each month for the Arizona Department of Corrections and Pima County jail since 2006. During that time as many as 16 sites within the Arizona prison system and one county jail were served by an infectious diseases specialist and pharmacist. Since the establishment of the clinic, we have consulted on thousands of incarcerated individuals (at any one time, the prison census was approximately 45,000 individuals). Until the onset of the recent pandemic, over 80% of the consultations involved HIV infection in its many stages of presentation and treatment. Beginning in January 2020 there was a sharp drop in the number of monthly consultations from 19/month to 7/month following the public health emergency regarding the SARS-CoV-2 pandemic. Only since ending the emergency have the number of consults risen to now, pre-pandemic numbers. However, the nature of consult requests has changed. In this report we document the change from predominately HIV consults to a broader spectrum of infection-related issues, most noteworthy being infective endocarditis, osteomyelitis, and chronic hepatitis B and C infection, almost all cases due to intravenous drug injection.
Methods
This is a retrospective descriptive study to characterize the number and characteristics of patients seen at the University of Arizona infectious diseases telemedicine clinics to the Arizona Department of Corrections (DOC) and Pima County Jail before, during and after the COVID-19 pandemic.
Record Review. Records of clinic visits from 2019 through April 2023 were obtained from the eMR of Banner University Medical Center, Tucson, AZ. Patient records were searched for age, sex, diagnoses, laboratory values, treatment, number of appointments, and outcomes. All patient data was de-identified.
Results
Telemedicine clinics for 2006-2020 were conducted in the University of Arizona telemedicine Program (ATP) utilizing state-of-the-art telephonic connections, cameras, and computers. It was conducted with an ATP engineer available to trouble shoot connections with the widely dispersed Arizona prison system. A separate connection was established with the Pima County Jail, which was terminated in 2021. With few exceptions a medical assistant or nurse on site controlled the camera link with the prison. The ATP clinic coordinator arranged patient visits with prison sites with Centurion, Sterling, VA through 2022 and in January 2023 onward, with NaphCare Western States Corporate Office, Las Vegas, NV. Patients were assigned to this consult clinic by physicians and nurses on site. The patients were seen in consultation for 20-30 minutes, and a clinic note entered into the medical record. Generally, laboratory values and medical records from the prison were faxed ahead of time. The telemedicine physician, pharmacist, and clinic coordinator were present during the clinic visit. However, at the start of the pandemic in January 2020, access to the hospital and University of Arizona School of Medicine were restricted and non-essential employees (including those of the ATP) were furloughed. The clinic was even cancelled on 5 occasions. Thereafter, HIPAA-compliant programs including Zoom (San Jose, CA) and eVisit (eVisit.com) were used to provide telemedicine patient care. The physician, pharmacist, and clinic director used their home computers to individually communicate with the DOC and jail.
Prior to the pandemic in 2019 there were 228 telemedicine clinic patients (19/month). That total was fairly representative of the yearly clinic visits by inmates prior to the SARS-CoV-2 pandemic. These numbers sharply declined to 7/month (307 total visits during the 40 months of the Public Health Emergency, January 2020 to May 2023). Clinic visit numbers have returned to pre-pandemic numbers only since expiration of the emergency pandemic measures. The drop in clinic numbers was undoubtedly due to a number factors including a change in prison personnel and the organizations providing medical care to the prisons. Masking of all personnel and spacing within the prison became a problem for telemedicine. It was difficult to move prisoners through cell blocks to the medical unit where telemedicine was available and some incarcerated individuals refused to attend telemedicine for this reason.
In addition to fewer patients during the pandemic, there was a change in the patients’ presenting problems. Prior to the pandemic >80% of the visits involved HIV infection, however, during the pandemic only 68 of 169 original patients (40%) had HIV infection and were seen at 213 visits (62.4% of total visits) (Table 1).
Table 1. Six most frequent diseases cared for by telemedicine clinic during SARS-CoV-2 pandemic. #: Human Immunodeficiency Virus; *: insufficient data provided to determine which valves were infected.
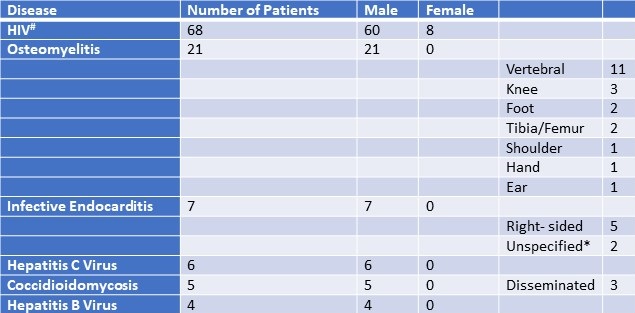
Similarly, 21 patients (12.4%) had osteomyelitis accounting for 37 total visits (12% of total visits). Of those 21 patients, 17 were admittedly or most likely associated with intravenous drug use (IVDU) while incarcerated and were cured of infection, 4 patients had chronic osteomyelitis (2 with coccidioidomycosis, 1 with diabetes and a foot infection, and one patient with congenital osteitis and recurrent infection of the inner ear). Seven patients were seen for infective endocarditis, all related to IVDU, and all judged clear of infection. The majority were infected with methicillin-sensitive Staphylococcus aureus. Ten patients were seen with hepatitis, 6 with HCV and 4 with HBV. Of those with HCV infection, all were recommended to begin therapy except one patient with cirrhosis and severe portal hypertension and hepatic cell carcinoma. All the HBV-infected individuals were controlled with nucleoside inhibitors.
Although the DOC and the jail underwent major upheavals intramurally due to the pandemic, the medical outcomes judging from the results with HIV patients were excellent. Only 1 of the 68 HIV-infected individuals seen had unaddressed resistance to anti-retroviral therapy (ART). The 67 other HIV patients, including 2 with interrupted therapy and 4 new arrivals to DOC were started on ART, demonstrated sustained viral suppression or are anticipated to do so by the next visit (thus, 98.5% achieved sustained viral suppression).
Discussion
UNAIDS has set a target of 2030 to eradicate HIV and has provided a timeline by which such an event may happen that includes diagnosing 95% of those who are infected with HIV, putting 95% of those on ART and achieving 95% viral suppression of those on ART (1). Similarly, The World Health Organization has announced plans to eliminate HBV and HCV by 2030 (2). Judging by the outcome data of our clinic even with the added stress of the recent SARS-CoV-2 pandemic, the DOC is doing their part in trying to eradicate these three diseases (Table 1). Prisoners are considered a vulnerable group at risk for 3 blood-borne viral infections, however, in the case of HIV at least, the DOC appears to be doing an excellent job in suppressing HIV even during the SARS-CoV-2 pandemic. The arrival of COVID 19 did not negatively affect the care of HIV (3). We found this to be true as well in our experience. HBV has long been controlled within the DOC using nucleosides, but HCV treatment is only now beginning in earnest in the Arizona DOC. At present we are seeing more HCV infections monthly than other infections. From our recent experience it appears that intravenous drug injection is the greatest infectious health risk among prisoners, not tuberculosis or other communicable diseases.
Telemedicine is an excellent modality for use in consults where the physician and patient are separated by great distances, such as are the many facilities of the DOC. It is more cost-effective for the DOC to use telemedicine than transporting prisoners to brick-and-mortar clinics (4). Specialty telemedicine clinics can be scheduled and the needed medical personnel assembled on video to see the patients (5) The only downside to telemedicine to the DOC was the infrequent occurrence of an inmate who showed for consultation but important laboratory and radiology reports were not available.
In conclusion, we have found that telemedicine clinics improve drug adherence among patients with HIV and may be superior to in-person visits with respect to treating and following patients with HIV (6). In addition, we found telemedicine clinics to be useful for the diagnosis, management and treatment of severe, life-threatening infectious diseases such osteomyelitis, infective endocarditis, HIV, hepatitis B and hepatitis C infections presenting in incarcerated patients.
References
- UNAIDS alerts countries to an unprecedented opportunity to stop new HIV infections, end AIDS and prepare for future pandemics. https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2023/may/20230524_PR_WHA_Prevention_en Accesse11 September 2023.
- World Health Organization. Global Health Sector Strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030 (GHSS). https://www.who.int/publications/i/item/9789240053779. Accessed 11 September 2023.
- Hanson HA, Kim E, Badowski ME. A Systematic Review: Impact of SARS-CoV-2 Infection on Morbidity, Mortality, and Viral Suppression in Patients Living With HIV. SN Compr Clin Med. 2023;5(1):144. [CrossRef] [PubMed]
- Esmaeili ED, Azizi H, Dastgiri S, Kalankesh LR. Does telehealth affect the adherence to ART among patients with HIV? A systematic review and meta-analysis. BMC Infect Dis. 2023 Mar 17;23(1):169. [CrossRef] [PubMed]
- Klotz SA, Jernberg JB, Robbins RA. Turn Healthcare Workers Loose with Outpatient telemedicine-Let Them Decide Its Fate; No Top-Down Decisions on What It Can and Cannot Do. Am J Med. 2023 May 23:S0002-9343(23)00341-8. [CrossRef] [PubMed]
- Klotz SA, Chan CB, Bianchi S, Egurrola C, York LD. The Genie Is Out of the Bottle: Telemedicine Is More Effective Than Brick-and-Mortar Clinics in the Care of HIV-Infected Outpatients. Am J Med. 2023 Apr;136(4):360-64. [CrossRef] [PubMed]
 Rick Robbins, M.D.
Rick Robbins, M.D.
Reader Comments