How Much Should Healthcare CEO’s, Physicians and Nurses Be Paid?
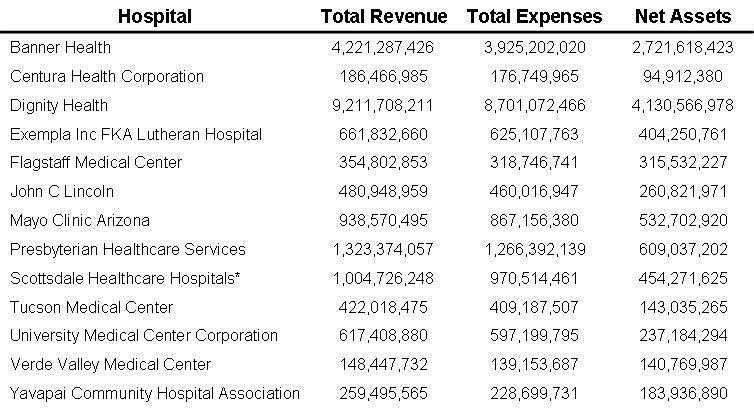
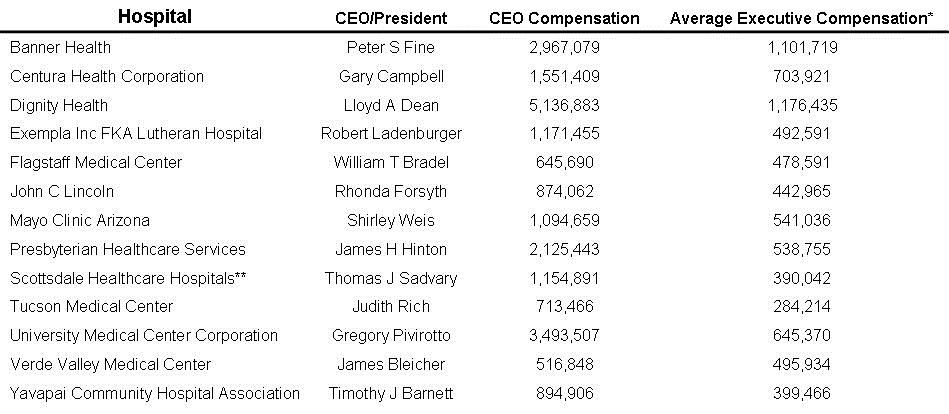
In 2019 the Southwest Journal published an editorial that stated one cause for the rising costs in healthcare was chief executive officer (CEO) compensation (1). Based on 2017 salaries, Peter Fine from Banner Health was the highest paid healthcare CEO in the country with compensation of $25.5 million. In comparison, the CEO of Mayo Clinic Arizona was paid a paltry $1.8 million (2). We decided to do a follow-up, and found that after a dip during the first year of the COVID-19 pandemic, Mayo raises resumed in 2021. Mayo’s CEO, Dr. Gianrico Farrugia, was paid $3.48 million in 2021 up from $2.74 million in 2020 (3). Dr. Richard Gray, CEO of the Mayo Arizona campus, was paid $1.78 million in 2021, up 26% from the previous year. I shared these numbers with a couple of the Mayo Clinic faculty who were surprised by the amount of compensation their executives were receiving.
Mayo Clinic posted $1.2 billion in net operating income in 2021 (3). More recently, the system reported net operating income of $157 million for the third quarter of 2022 with an operating margin of 3.8 percent. Compensation for Mayo Clinic executives is set by the Mayo Clinic Salary & Benefits Committee and endorsed by the Mayo Clinic Board of Trustees Compensation Committee. Mayo claims not to be a profit-sharing institution and that pay is not linked to doing anything more or less for the patient than what is needed. It is unclear how CEO compensation in the millions fits with this patient care philosophy.
I did a preliminary survey of physicians in the Phoenix area of how much healthcare CEOs should be paid. Not surprisingly, most of these physicians thought that CEOs should be physicians like they are at the Mayo Clinic. Opinions on CEO compensation were all over the board. However, the best answer, in my opinion, came from a retired ID physician. He thought CEOs should be well compensated but should be paid less than senior physicians. His reasoning was that patients come to the Mayo Clinic or other healthcare organizations not because of the CEO, but because of Mayo’s physicians. Lawyers have this figured this out. One of my closest friends is an administrative partner for a large (over 100 lawyers) law firm in Phoenix. He said he is well compensated but paid less than his senior partners. The reasoning was much the same. Clients come not because of his administrative skills, but because of the lawyers. However, he was quick to point out that managing partners do deserve some compensation for their lost income in not practicing law. The compensation committee in these cases is the senior partners.
Some would argue that certain physicians are over-paid. I would agree. Current fee-for-service payment rates for physician visits trace back to the origins of Blue Cross Blue Shield (BC/BS) insurance in the 1930s. At that time, BC/BS rates were set to pay generously for hospitalizations and operations. Payments for so-called “cognitive services” were lower. In the 1960’s Medicare adopted the BC/BS payment model. This disparity has been perpetuated through “Relative Value Units”. Despite recognition by the Medicare Payment Advisory Commission (MedPAC) of the adverse effects of inadequate payment to some physicians, especially primary care, only limited progress has been made toward correction of the disparity (4). This may be due, at least in part, to treatment of total payment for physicians as a zero-sum game in which decision making is dominated by non–primary care physicians through mechanisms such as the Relative Value Scale Update Committee (RUC) (5). This translates to hospitals, procedure-oriented specialties, and especially some surgical subspecialties compensated in excess compared to more cognitive specialties.
When BC/BS was founded in 1929, one goal of the American healthcare Association (AHA) and the American College of Surgeons was to eliminate the “Doctor’s Hospitals”. These physician-run hospitals were sometimes substandard. However, little progress in eliminating them was made until establishment of Medicare and Medicaid in 1965. Many of the “Doctor’s Hospitals” did not meet criteria for Medicare certification. Lack of Medicare and Medicaid payments essentially closed their doors. However, the doctor run hospitals are now making a comeback through surgical centers. Although the AHA has questioned their quality, most have matched or exceeded the quality metrics used by the Joint Commission or other groups and often score better than hospitals in head-to-head comparisons (6). Doctors who run such centers deserve some payment for their administrative efforts.
Nurse practitioners (NPs) and physician assistants (PAs) serve a vital role in patient care. They deserve to be well paid. However, their education and responsibility are generally less than physicians. For example, 1000 clinical hours are required for nurse practitioner certification which represented about 10 weeks of my internship or about 13 weeks under the current 80-hour work week limit. Similarly, PAs are required to only complete 1600 hours of clinical training. In contrast, physicians complete family practice, internal medicine, or pediatric residencies which require a minimum of 3 years, with most subspecialities requiring an additional 3+ years. Surgical residencies are usually 5 years. Furthermore, there appears to me more risk assumed by a physician. In 2019 there were only 420 malpractice suits filed against nurse practitioners and PAs compared to over 20,000 total medical malpractice suits (7).
Nurses are the backbone of any healthcare organization. Although they usually have less education than physicians, NPs, or PAs, nursing is intense and stressful with nurses assuming a large responsibility and delivering the most beside care. Because patients are close at hand, nurses often make independent care decisions. In Arizona, nurse compensation averaged about $78,330 in 2019 (8). Not surprisingly it is considerably higher in California where the cost of living is higher compensation and averages $113,240. Recently, more nurses are working as traveling nurses, or filling a staffing shortage at a hospital or healthcare facility on a temporary basis. Prior to COVID-19 many nurses were dissatisfied with healthcare working conditions (8). This suggests that nurses may be seeking other employment options that provide them with more control over where and when they work (9). Travel nursing provides these options at a higher pay.
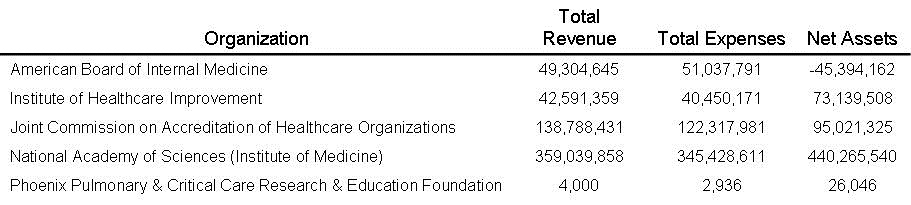
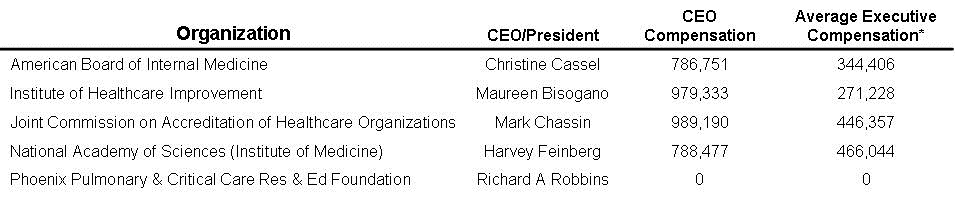
The causes of the overcompensation of CEOs at the expense of historically undercompensating some nurses and physicians have been salary and benefits committees set up under a corporate structure. Under the present system of healthcare governance an executive board appointed or heavily influenced by a CEO appoints a board which appoints a salary and benefits committee. The later committee in turn sets salary and benefits for the organization including the executives. A compensation committee consisting of physician and nursing leaders could more realistically evaluate an individual’s value to a healthcare organization. However, it seems likely that such a change will require mandates from healthcare certifying organizations. Healthcare executives are unlikely to readily relinquish the present system which has rewarded them so generously. Therefore, physicians need to lobby various organizations such as the Joint Commission, the Relative Value Scale Update Committee (RUC), ACGME, etc. for a compensation system which examines administrative efficiency and addresses areas of administrative complexity that add costs to the health care system without improving accessibility or value. This is in contrast to the present system of rewarding those who serve a for-profit corporate structure rather than improving healthcare in a not-for-profit system.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Robbins RA. CEO compensation-one reason healthcare costs so much. Southwest J Pulm Crit Care. 2019;19(2):76-8. [CrossRef]
- Innes S. This Arizona nonprofit health system CEO topped the salary list at $25.5 million in 2017. Arizona Republic, October 23, 2019. Available at: https://pnhp.org/news/this-arizona-nonprofit-health-system-ceo-topped-the-salary-list-at-25-5-million-in-2017/ (accessed 1/16/23).
- Gamble M. Mayo Clinic defends executive raises. Becker’s healthcare Review. Dec. 8, 2022. Available at: https://www.beckers healthcarereview.com/compensation-issues/mayo-clinic-defends-executive-raises.html ((1/17/23).
- MedPac. March 2022 Report to the Congress: Medicare Payment Policy. March 2022. Available at: https://www.medpac.gov/document/march-2022-report-to-the-congress-medicare-payment-policy/ (accessed 2/4/23).
- Magill MK. Time to Do the Right Thing: End Fee-for-Service for Primary Care. Ann Fam Med. 2016 Sep;14(5):400-1. [CrossRef] [PubMed]
- Pham N, Donovan M. The Economic and Social Benefits of Physician-Led Hospitals. ADP Analytics. September 2022. Available at: https://ndpanalytics.com/wp-content/uploads/PHA-Economic-Impact-Report-092022-Final-R1.pdf (accessed 2/3/23).
- Chesney S. Do Nurse Practitioners Really Get Sued? Berxi. Aug 16, 2021. Available at: https://www.berxi.com/resources/articles/do-nurse-practitioners-get-sued/ (accessed 2/3/23).
- 2U Inc. Nurse Salary. Available at: https://nursinglicensemap.com/resources/nurse-salary/ (accessed 2/3/23).
- Yang YT, Mason DJ. COVID-19’s Impact On Nursing Shortages, The Rise Of Travel Nurses, And Price Gouging. Health Affairs Forefront. January 28, 2022. Available at: https://www.berxi.com/resources/articles/do-nurse-practitioners-get-sued/https://www.healthaffairs.org/do/10.1377/forefront.20220125.695159/ (accessed 2/3/23).
Cite as: Robbins RA. How Much Should Healthcare CEO’s, Physicians and Nurses Be Paid? Southwest J Pulm Crit Care Sleep. 2023;26(2):24-27. doi: https://doi.org/10.13175/swjpccs007-23 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.