
Combating Physician Moral Injury Requires a Change in Healthcare Governance
One of our associate editors, Mike Gotway, emailed me an editorial titled “Burnout versus Moral Injury and the Importance of Distinguishing Them” from Radiographics authored by Sara Sheikhbahaei and colleagues (1). It is well worth reading the full text. However, since Radiographics is not an open access journal and the full text is not available to everyone, I will do my best to summarize Sheikhbahaei’s editorial and expand where appropriate. Nearly every journal (including the SWJPCCS) has published an article and/or editorial on physician burnout. Sheikhbahaei (1) points out that physician burnout is different than moral injury. She uses Talbot and Dean’s (2) definition of burnout as “a pattern of exhaustion, cynicism, and decreased productivity often accompanied by anxiety, cognitive impairment, and diminished functional capacity”. Her editorial points out that “the consequences of burnout are serious and include depression, stress, increased risk of substance abuse, poor self-image, lack of motivation, decreased productivity, poor employee retention, and loss of reputation for the institution”. However, she is also quick to point out that there are corrective measures available, and burnout is generally reversible.
Like post-traumatic stress disorder (PTSD), moral injury was first described in post-war veterans but is now being expanded to non-veterans and non-military situations. Johnathan Shay (3), who introduced the concept of moral injury as a distinct syndrome differing from PTSD, defined moral injury as occurring when: (a) there has been a betrayal of what is morally right, (b) by someone who holds legitimate authority and (c) in a high-stakes situation. Shay went on to describe moral injury creation as "leadership malpractice".
What distinguishes moral injury from burnout is that it is generally irreversible (1). “The most grievous consequences of moral injury are (a) loss of institutional loyalty (or worse, loss of loyalty to medicine in general), and (b) detachment from the noble ideas that attracted one to medicine in the first place. Such heavy soul wounds leave permanent scars and can cause lifelong feelings of betrayal by the institution. Corrective measures (e.g., changing jobs, increasing vacation time or remuneration, providing psychologic support) may mitigate burnout but cannot heal the permanent wounds of moral injury” (1).
The Radiographics editorial points out that in academic medicine ethical standards are violated by the very entity that instilled them in the first place — academic medicine (1). The tripartite mission of academic medicine (patient care, teaching, and research) has been increasingly supplanted by institutional priorities that focus on control of the clinical practice of physicians; the production and distribution of medicine; and the redistribution of its financial productivity away from the original objectives (1). Academic medicine had been a calling for professionals willing to sacrifice financial gain while seeking fulfillment in research and teaching. This has changed, not because the physicians changed, but because academic medicine changed.
Institutional priorities have diverged from those of physicians and are nearly exclusively molded by financial considerations (1). Countless metrics of dubious relevance, measurement of physician worth by clerical skills and other myopic administrative efforts detract from academic medicine’s true calling of providing the best patient care, education and research. Health care administration has pursued a business culture to cement administration’s fiscal goals. Worse than simply wasting resources, administration punishes physicians who rebel against their financial structure. To avoid this losing conflict, physicians may impose self-censorship, settle on a daily routine of doing the minimum required to get by, or simply resign. The coup de grace is the feeling of deep betrayal that becomes permanently fixed. It is the physicians’ training at these very institutions that etched the primary moral creed of serving the patient. Now, these same institutions demand that physicians devalue this deeply held moral belief and toe the line for institutional financial gain.
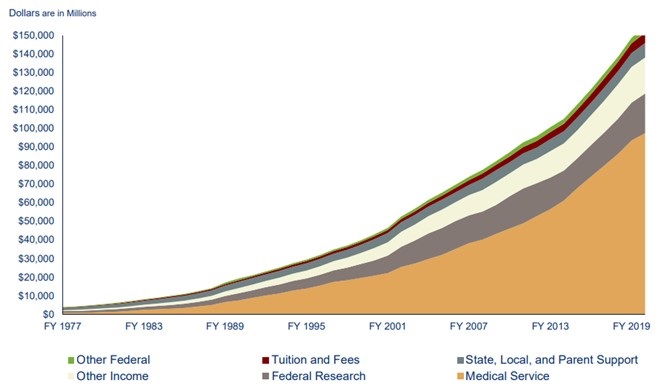
It is the administration of the institution, and the bureaucracy that results, that causes, defends, grows, and perpetuates physician moral injury. The growth of the administrative bureaucracy is staggering. Between 1975 and 2010, the number of physicians in the United States grew by 150%, but the number of health care administrators grew by 3200% (4). In 2019, Sahini (5) estimated that the United States spent nearly 25% or $1 trillion directly on healthcare administration with some believing that adding the indirect costs makes the true costs closer to 40% (6). These numbers are the source of the old joke from a couple of decades ago that in the future not everyone will have a doctor or nurse but everyone will have an administrator. Unfortunately, that time has arrived.
Sheikhbahaei (1) states that institutions should educate administrators away from emphasizing financial gain to emphasizing excellence in patient care by facilitating clinical practice. Some administrators do, others do not. Resources should be redirected from bureaucratic efforts of little value toward improving health care quality and accessibility, reversing a long-standing trend in the other direction. Those who deliver health care should be shielded from unnecessary tasks. According to Sheikhbahaei this can be achieved by delegating to clinicians some oversight of the medical bureaucracy (1). Although I agree with the sentiment, I disagree with the lack of action. Merely pointing out that there is a problem is not likely to solve it, especially when the beneficiaries of the present system, the administrators, are charged with fixing it. We need to do more than identify and study areas of administrative complexity that add costs to healthcare but do not improve value or accessibility. Administrators have taken the money and run, squandering their chance to deliver quality care at lower prices. Prior to the 1980’s physicians were mostly in charge and did better — they can do better again. However, first they need control. Physicians should demand that regulatory organizations such as the Joint Commission, Centers for Medicare and Medicaid, ACGME, etc. remove administrators from control of healthcare. Regulators need to address policies that add costs without patient benefit or improvement in education and research. Leaving healthcare administrators in charge without oversight and accountability will preserve the present system of substandard healthcare, poor accessibility, deficient education, second-rate research, high prices, and “leadership malpractice”.
Richard A. Robbins, MD
Editor, SWJPCCS
References
- Sheikhbahaei S, Garg T, Georgiades C. Physician Burnout versus Moral Injury and the Importance of Distinguishing Them. Radiographics. 2023 Feb;43(2):e220182. [CrossRef] [PubMed]
- Talbot SG, Dean W. Physicians are not “burning out”. They are suffering from
- moral injury. STAT. https://www.statnews.com/2018/07/26/physicians-not-burning-out-they-are-suffering-moral-injury/ (accessed 2/14/23).
- Shay J, Munroe J. Group and Milieu Therapy for Veterans with Complex Posttraumatic Stress Disorder. In: Saigh, PA, Bremner JD, eds. Posttraumatic Stress Disorder: A Comprehensive Text. Boston: Allyn & Bacon; 1998:391-413.
- Cantlupe J. Expert Forum: The rise (and rise) of the healthcare administrator. November 7, 2017. Available at: https://www.athenahealth.com/knowledge-hub/practice-management/expert-forum-rise-and-rise-healthcare-administrator (accessed February 6, 2023).
- Sahni NR, Mishra P, Carrus B, Cutler DM. Administrative Simplification: How to Save a Quarter-Trillion Dollars in US Healthcare. McKinsey & Company. October 20, 2021. Available at: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/administrative-simplification-how-to-save-a-quarter-trillion-dollars-in-US-healthcare (accessed 2/6/23).
- Robbins RA, Natt B. Medical image of the week: Medical administrative growth. Southwest J Pulm Crit Care. 2018;17(1):35. [CrossRef]
Cite as: Robbins RA. Combating Physician Moral Injury Requires a Change in Healthcare Governance. Southwest J Pulm Crit Care Sleep. 2023;26(3):34-6. doi: https://doi.org/10.13175/swjpccs008-23 PDF
 Rick Robbins, M.D.
Rick Robbins, M.D.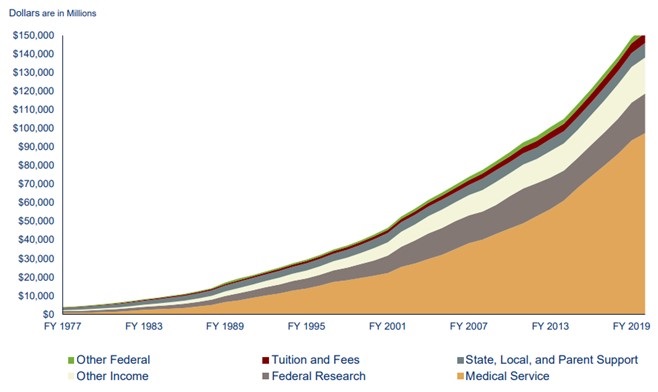
{kind=link}