
Utility of Endobronchial Valves in a Patient with Bronchopleural Fistula in the Setting of COVID-19 Infection: A Case Report and Brief Review
Nazanin Sheikhan, MD1, Elizabeth J. Benge, MD1, Amanpreet Kaur, MD1, Jerome K Hruska, DO2, Yi McWhorter DO3, Arnold Chung MD4
1Department of Internal Medicine, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
2Department of Pulmonology, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
3Department of Anesthesiology Critical Care Medicine, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
4MountainView Cardiovascular and Thoracic Surgery Associates, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
Abstract
Patients with COVID-19 pneumonia frequently develop acute respiratory distress syndrome (ARDS), and in severe cases, require invasive mechanical ventilation. One complication that can develop in patients with ARDS who are mechanically ventilated is a bronchopleural fistula (BPF). Although rare, the frequency of BPF in patients with COVID-19 pneumonia is increasingly recognized. Here, we present a 48-year old man with BPF associated with COVID-19 pneumonia. Treatment with a commercial endobronchial valve (EBV) system resulted in reduced air leak allowing for tracheostomy placement. Our case adds to a growing body of evidence suggesting that the presence of COVID-19 pneumonia does not hinder the utility of EBV’s in the treatment of BPF’s.
Abbreviation List
- ARDS = acute respiratory distress syndrome
- BIPAP = Bilevel Positive Airway Pressure
- BPF = Bronchopleural Fistula
- COVID-19 = Coronavirus Disease-2019
- CT = Computed Tomography
- CTA = Computed Tomography Angiography
- EBV = Endobronchial Valve
- HFNC = High Flow Nasal Cannula
- ICU = Intensive Care Unit
- RML = Right Middle Lobe
- RUL = Right Upper Lobe
- SARS-CoV-2 = Severe Acute Respiratory Syndrome Coronavirus-2
- VATS = Video-Assisted Thoracoscopic Surgery
Introduction
The COVID-19 pandemic has resulted in over one hundred million infections worldwide, in addition to millions of deaths (1). A less common sequelae of COVID-19 is bronchopleural fistula (2). A bronchopleural fistula is an abnormal sinus tract that forms between the lobar, main stem, or segmental bronchus, and the pleural space (3). BPF is typically treated by surgical repair, via a video-assisted thoracoscopic surgical approach (VATS) (3). Bronchoscopic approach with placement of airway stents, coils or transcatheter occlusion devices can be considered for those who are not suitable for surgical intervention (3). A newer therapeutic modality for bronchopleural fistulae are endobronchial valves, which have been used successfully to treat COVID-19 patients diagnosed concurrently with bronchopleural fistulae (4).
Here, we present a case of a critically ill patient developing a bronchopleural fistula with a concurrent COVID-19 infection, whose respiratory status was stabilized with an endobronchial valve. To our knowledge, this is one of four case reports of a bronchopleural fistula arising in the setting of COVID-19.
Brief Review of Endobronchial Valves in COVID-19
Several other studies report success using endobronchial valves to treat bronchopleural fistulae in patients with COVID-19 pneumonia. One case series documents two cases of COVID-19 pneumonia complicated by bacterial super-infections, in which both patients experienced pneumothorax and persistent air leaks after mechanical invasive ventilation. Both patients were successfully treated via EBV positioning. These researchers speculate that the severe inflammation associated with COVID-19 related ARDS induces inflammatory-related tissue frailty, pre-disposing lung tissue to damage via barotrauma, and the subsequent development of BPF (5).
Another case documents the treatment of a 49-year-old male with COVID-19 pneumonia who was treated with steroids and tocilizumab. He also had a 3-week history of persistent air leak, which was successfully treated with an EBV. This team emphasizes that the thick, copious sections evident in patients afflicted by COVID-19 pose a risk for EBV occlusion. They highlight the importance of medically optimizing the patient and draining the air leak to mitigate the potential of this procedural complication developing (4).
In conjunction with the treatment course presented in our case, these case reports provide compelling evidence indicating that endobronchial valves can be successfully used to treat persistent air leaks in patients with COVID-19 pneumonia.
Case Presentation
Our patient is a 48-year-old male with a medical history significant for essential hypertension and Type 1 diabetes mellitus who presented to the emergency department complaining of acute onset generalized weakness, shortness of breath, and a near-syncopal event that had occurred the day prior. Vital signs on admission showed an oxygen saturation of 86% on ambient air, respiratory rate of 18 breaths per min, heart rate of 111 beats per min with a temperature of 37.6°C. He was tested for SARS-CoV-2 on admission and was found to be positive.
Initial computed tomography (CT) chest showed diffuse bilateral ground-glass opacities compatible with COVID-19 pneumonia. On admission, his inflammatory markers were elevated, with C-reactive protein 4.48 mg/dL, ferritin 1230 ng/ml, lactate dehydrogenase 281 IU/L, and D-dimer 0.76 mg/L. He received 1 dose of tocilizumab, convalescent plasma, as well as 5-day course of Remdesivir. His oxygen requirement increased as well as his work of breathing requiring High Flow Nasal Cannula (HFNC) and subsequently Bilevel Positive Airway Pressure (BiPAP); patient was transferred to the medical intensive care unit (ICU) 17 days after admission requiring intubation. Computed tomography angiography (CTA) chest could not be obtained to rule out pulmonary embolism as patient was too unstable. Patient was started on Heparin drip empirically which had to be discontinued due to gastrointestinal bleeding. He had worsening oxygenation, ventilator asynchrony, with P:F ratio of 47, requiring high-dose sedation and neuromuscular blockade, as well as prone positioning. Repeat CT chest on day 21 demonstrated bilateral pneumothoraces and pneumomediastinum as well as interval worsening of diffuse ground glass infiltrates (Figure 1), requiring bilateral chest tube placement.
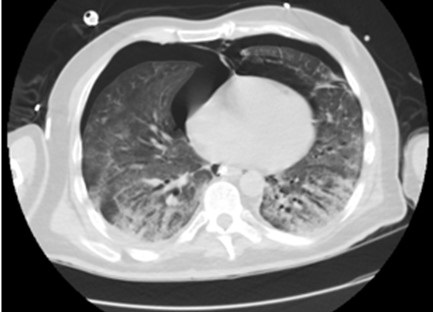
Figure 1. Computed tomography chest showing pneumomediastinum, bilateral pneumothoraces, and diffuse ground glass attenuation of the lungs bilaterally.
On the 34th day of admission, he developed a right-sided tension pneumothorax likely secondary to ongoing severe ARDS, requiring replacement of dislodged right chest tube. Patient subsequently had worsening of right pneumothorax requiring an additional second chest tube placement. Patient developed persistent air leak concerning for right bronchopleural fistula. On hospital day 42, patient underwent intrathoracic autologous blood patch with persistence of large air leak. After interdisciplinary conference with cardiothoracic surgery, pulmonary, and the ICU team, it was decided that patient is not a surgical candidate hence interventional pulmonology was consulted for EBV placement to facilitate chest tube removal and ventilator weaning.
Patient underwent fiberoptic bronchoscopy on hospital day 52; pulmonary balloon was used to sequentially block the right mainstem, bronchus intermedius, and basilar segments. The air leak was recognized to be coming from right middle lobe (RML) and the apex of the right upper lobe (RUL) status post placement of two endobronchial valves in the medial and lateral segments of the RML (Figure 2).
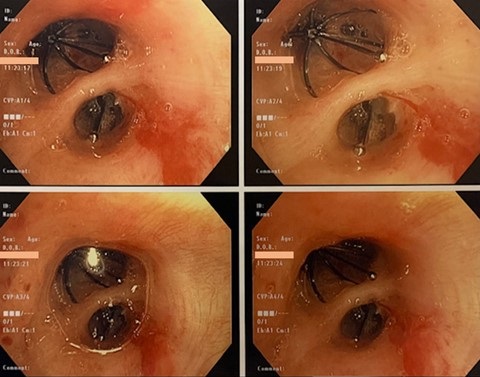
Figure 2. Bronchoscopic view of endobronchial valves.
The RUL could not be entered secondary to angulation and technical inability of the instruments to achieve a sharp bend. Post-bronchoscopy, patient had 50 mL reduction in air leak resulting in improvement of his ventilator settings such that a tracheostomy could be safely performed. Left-sided chest tube was removed with resolution of pneumothorax. Repeat CT chest on hospital day 115 demonstrated persistent right bronchopleural fistula (Figure 3).
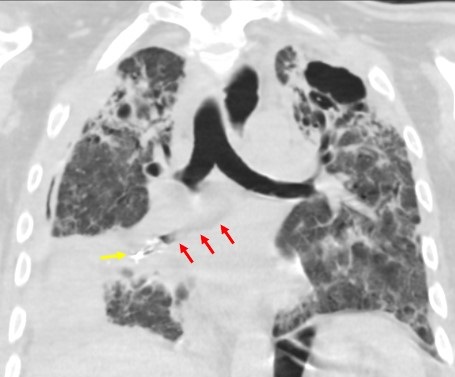
Figure 3. Computed tomography chest showing bronchopleural fistula in the right middle lobe and collapsed and shrunken right middle lobe with endobronchial occlusion stents at the central airway. Yellow arrow showing endobronchial valves and red arrows showing bronchopleural fistula
The patient is currently pending transfer to a long-term acute care hospital for aggressive physical therapy and eventual transfer to a tertiary center for lung transplantation evaluation.
Discussion
Scientific research has moved at an unprecedented speed in an attempt to shed light on the manifestations of COVID-19. The most common presentation of COVID-19 includes cough, fever, shortness of breath, and new onset anosmia and ageusia (6).
Common complications include coagulopathy, pulmonary emboli, and in severe cases, acute respiratory distress syndrome (7). Bronchopleural fistulae have emerged as a rare but known complication of COVID-19. This pathology is traditionally seen as a post-surgical complication arising from lobectomy or pneumonectomy (8). All cause mortality secondary to bronchopleural fistulae are high; with mortality rates ranging from 18-67% (8).
A relatively novel therapeutic modality for bronchopleural fistulae are endobronchial valves, which have been used in patients who are not candidates for surgery, such as our patient (9). They work as a one-way valve that allow the pathologically trapped air to exit the respiratory system, but not enter (4).
Differential diagnoses for bronchopleural fistulae include alveolar pleural fistulas and empyema (11). Alveolar pleural fistulas are abnormal communications between the pulmonary parenchyma, distal to a segmental bronchus, and the pleural space, while bronchopleural fistulas are more proximal; representing abnormal connections between a mainstem, lobar, or segmental bronchus and the pleural space (12). These pathologies are differentiated with direct visualization on bronchoscopy, as was demonstrated in our patient (12).
There are currently no official statistics on the epidemiology of bronchopleural fistulae in COVID-19. A disappointing aspect of our case was the lack of complete resolution of the patient’s air leak after the placement of the endobronchial valve. While the patient’s condition did improve after the valve was placed, he continued to suffer from respiratory illness related to his bronchopleural fistula. Although complete remission was not achieved, the endobronchial valve placement did facilitate respiratory recovery sufficient enough to facilitate a tracheostomy. The patient was then stabilized for eventual transfer to a long-term acute care facility, where he will undergo physical therapy and await lung transplantation. It is important to emphasize that while the endobronchial valve was not curative, it stabilized the patient for possible future curative treatments.
Conclusion
Despite their rarity, bronchopleural fistulas are a pulmonary complication of COVID-19. Although the insertion of the endobronchial valve in our patient resulted in a reduction of the air leak as opposed to complete resolution, this case still emphasizes a therapeutic benefit of endobronchial valves in such instances. Overall, our case demonstrates the importance of clinical vigilance in the face of unusual pulmonary complications related to COVID-19, and that treatment of these complications requires flexibility and creativity.
References
- WHO Coronavirus (COVID-19) Dashboard [Internet]. World Health Organization. World Health Organization; [cited 2021May31]. Available from: https://covid19.who.int/
- Hopkins C, Surda P, Kumar N. Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology. 2020 Jun 1;58(3):295-298. [CrossRef] [PubMed]
- Miesbach W, Makris M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620938149. [CrossRef] [PubMed]
- Talon A, Arif MZ, Mohamed H, Khokar A, Saeed AI. Bronchopleural Fistula as a Complication in a COVID-19 Patient Managed With Endobronchial Valves. J Investig Med High Impact Case Rep. 2021 Jan-Dec;9:23247096211013215. [CrossRef] [PubMed]
- Donatelli P, Trenatacosti F, Pellegrino MR, et al. Endobronchial valve positioning for alveolar-pleural fistula following ICU management complicating COVID-19 pneumonia. BMC Pulm Med. 2021 Sep 27;21(1):307. [CrossRef] [PubMed]
- Salik I, Vashisht R, Abramowicz AE. Bronchopleural fistula. StatPearls [Internet]. 2020 Aug 27. [CrossRef]
- Cardillo G, Carbone L, Carleo F, Galluccio G, Di Martino M, Giunti R, Lucantoni G, Battistoni P, Batzella S, Dello Iacono R, Petrella L, Dusmet M. The Rationale for Treatment of Postresectional Bronchopleural Fistula: Analysis of 52 Patients. Ann Thorac Surg. 2015 Jul;100(1):251-7. [CrossRef] [PubMed]
- Sarkar P, Chandak T, Shah R, Talwar A. Diagnosis and management bronchopleural fistula. Indian J Chest Dis Allied Sci. 2010 Apr-Jun;52(2):97-104. [PubMed]
- Pathak V, Waite J, Chalise SN. Use of endobronchial valve to treat COVID-19 adult respiratory distress syndrome-related alveolopleural fistula. Lung India. 2021 Mar;38(Supplement):S69-S71. [CrossRef] [PubMed]
- Musani AI, Dutau H. Management of alveolar-pleural fistula: a complex medical and surgical problem. Chest. 2015 Mar;147(3):590-592. [CrossRef] [PubMed]
- Mehta HJ, Malhotra P, Begnaud A, Penley AM, Jantz MA. Treatment of alveolar-pleural fistula with endobronchial application of synthetic hydrogel. Chest. 2015 Mar;147(3):695-699. [CrossRef] [PubMed]
Acknowlegements
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Cite as: Sheikhan N, Benge EJ, Kaur A, Hruska JK, McWhorter Y, Chung A. Utility of Endobronchial Valves in a Patient with Bronchopleural Fistula in the Setting of COVID-19 Infection: A Case Report and Brief Review. Southwest J Pulm Crit Care. 2021;23(4):109-14. doi: https://doi.org/10.13175/swjpcc046-21 PDF
 Post a Comment
Post a Comment
Reader Comments