Evan Denis Schmitz, MD
Robert A. Raschke, MD
Good Samaritan Regional Medical Center/Phoenix Veteran Affairs Medical Center Phoenix, AZ
Refernce as: Schmitz ED, Raschke RA. A 32 year old male with idiopathic hepatic encephalopathy and necrotic lower extremity. Southwest J Pulm Crit Care 2010;1:14-20. (Click here for PDF version)
Abstract
A 32 year old with undiagnosed alpha-1 antitrypsin deficiency had an unusual initial presentation of acute liver failure, septic shock; adult respiratory distress syndrome and what appeared to be a left lower extremity soft tissue infection. Skin biopsy revealed panniculitis. Because of the diagnosis of panniculitis, an alpha-1 antitrypsin level was ordered and demonstrated alpha-1 antitrypsin deficiency with a ZZ phenotype. The patient recovered with antibiotics and supportive therapy. This case illustrates that alpha-1 antitrypsin deficiency can present other that the more usual adult presentation of progressive emphysema. Unexplained panniculitis should prompt investigation of alpha-1 antitrypsin deficiency in the adult patient.
Case Presentation
History of Present Illness
A 32 year old male was admitted to an outside hospital altered mental status and respiratory failure requiring intubation. He was diagnosed with liver failure and a lower extremity soft tissue infection. He developed E. coli bacteremia and septic shock. He was transferred to Good Samaritan Regional Medical Center. Two months prior to admission he developed diarrhea as well as bilateral lower extremity edema. Odd behavior was reported by co-workers. His skin became pale then yellow. There was no significant past medical history. There was no family history of liver or lung disease. He drank 3 beers a day but denied any tobacco or illicit drug use. He was using supplements such as creatine, rip fuel and energy drinks for over a year. He denied any anabolic steroid use.
Physical Examination
On arrival to the ICU his vitals were as follows: blood pressure of 88/30, heart rate of 103 and a respiratory rate of 35. He was obtunded and intubated. He had scleral icterus. He was tachycardic with no murmurs, rubs or gallops. He was tachypneic with diminished breath sounds bilaterally. Abdomen was distended with fluid shift. He had 4+ pitting edema and necrosis of his left leg (Figure 1).

Figure 1. Left Leg
Laboratory Findings
Arterial blood gas revealed a pH of 7.05, PaCO2 of 37 mmHg and a PaO2 of 260 mmHg. Hemogram showed a white blood cell count of 6.9 cells/µL, hemoglobin of 6.5 g/dL and platelet count of 289,000 cells/µL. Serum chemistry results were sodium of 123 mEq/L, potassium of 4.2 mEq/L, chloride of 93 mEq/L, bicarbonate of 9 mEq/L, urea nitrogen of 33 mg/dL, creatinine of 2.5 mg/dL, glucose of 51 mg/dL, lactic acid level of 9.2, ammonia of 58 mg/dL, total bilirubin of 2.2 mg/dL, , albumin of 1.4 g/dL, aspartate aminotransferase of 77 U/L and an alanine aminotrasferase of 65 U/L (normal ranges10-60 and 10-50 respectively). Alkaline phosphatase was normal. . Coagulation study results revealed an international normalized ratio of 2.1 and a partial thromboplastin time of 44.9 seconds. Hepatitis serologies were negative. Urinalysis was positive for bilirubin and a specific gravity of 1.020. Blood cultures grew E. coli.
Radiography
Chest X-ray revealed diffuse bilateral lower lobe consolidations in the lower lobes (see Figure 2). A CT scan was interpreted as not showing any significant emphysema.

Figure 2. Chest Radiography
Hospital Course
The patient’s vitals signs stabilized with the use of pressor medications and antibiotics. The lower extremity was debrided and skin biopsies were sent to pathology which confirmed inflammation and tissue necrosis (Figure 3, see arrows).
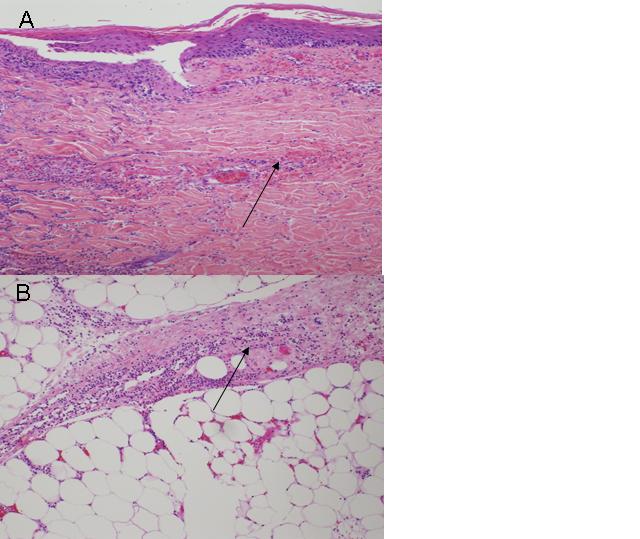
Figure 3. Skin biopsy (H&E staining).
Because of the panniulitis observed on the skin biopsy, a serum α-1 antitrypsin level was obtained which revealed a level less than 30 mg/dL. Genetic testing was also performed and the patient’s phenotype was identified as PIZZ.
Discussion
Manifestations of α-1 antitrypsin deficiency include emphysema, hepatic disease, panniculitis, vascular disease, inflammatory bowel disease, glomerulonephritis, and ANCA-positive vasculitis (1). Less than 50 cases of panniculitis have been reported (4). Panniculitis is not associated with any particular alpha-1 allele. There are many causes of panniculitis including Weber-Christian Disease, physical injury, multiple rheumatologic disorders, malignancies, dermatologic disorders, infections and several miscellaneous diseases including sarcoidosis in addition to alpha-1 antitrypsin deficiency. Necrotizing panniculitis in alpha-1 antitrypsin deficiency is caused by unopposed proteolysis in the skin which leads to lobular fat necrosis of the lower reticular dermis (4). Patients develop a hot and painful red nodule or plaque that may progress to necrosis if left untreated. Some have advocated alpha-1 replacement therapy for treatment of alpha-1 associated panniculitis (4).
Liver disease is caused by polymerization of the variant α-1 antitrypsin protein which results in intrahepatocyte accumulation and is an unusual presentation in the adult (2,3). PIZZ is the most common phenotype (1-3).
Conclusion
Presentation of alpha-1 antitrypsin deficiency with panniculitis E. coli bacteremia and ARDS is unusual. Most adults present with signs and symptoms of emphysema (1). He was successfully treated with positive pressure ventilation, antibiotics and supportive care and eventually left the hospital. It is unclear what precipitated his acute illness.
References
1. American Thoracic Society/European Respiratory Society Statement: Standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med 2003;168:818-900.
2. Teckman JH, Qu D, Perlmutter DH. Molecular pathogensis of liver disease in alpha-1 antitrypsin deficiency. Hepatology 1996;24:1504-16.
3. Perlmutter DH, Brodsky JL, Balistreri WF, Trapnell BC. Molecular pathogenesis of alpha-1 antitrypsin deficiency associated liver disease: a meeting review. Hepatology 2007; 45:1313-23.
4. Stoller JK and Pilang M. Panniculitis in alpha-1 antitrypsin deficiency: a review. Clin Pulm Med 2008; 15:113-7.
Presented at the Arizona Thoracic Society April 20, 2010 in Scottsdale, AZ and the Great Cases Session at the American Thoracic Society International Conference, May 16, 2010 in New Orleans, LA. A link to the slides used for these presentations is below.