
Correct!
5. All of the above
The clinical course of angiostrongyliasis is usually improvement even without specific treatment. Mortality rate is low at around 0.5 % (4). People infected with rat lung worm have pulmonary infiltrates which improve with clinical improvement of the patient (1).
In our opinion, the neurologic symptoms in this patient were sufficiently severe to warrant treatment. Oral albendazole and prednisone were begun on day two of the admission (9,10). Both medications were continued for 2 weeks. During the second week of her hospitalization PCR results from the CDC were reported as positive for Angiostrongylus. The patient slowly improved clinically with resolution of her headache in 4-5 days. Her lower extremity weakness improved over the next 4 weeks but needed ongoing rehabilitation at the time of discharge. She spent one month in a rehab facility and was eventually discharged home. Follow up chest CT three weeks after admission showed near complete resolution of her lung infiltrates which coincided with her clinical Improvement (Figure 4).
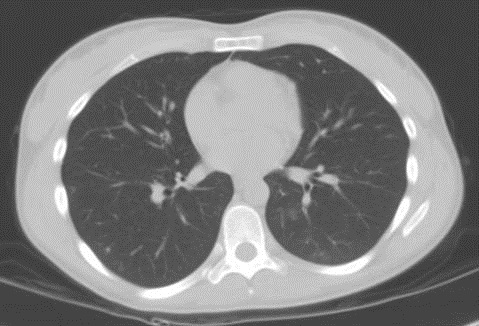
Figure 4. Thoracic CT scan three weeks after presentation.
This case illustrates the classic history, clinical presentation and lung imaging findings of Angiostrogylus cantonensis with confirmed diagnosis by PCR.
References
- Wang QP, Lai DH, Zhu XQ, Chen XG, Lun ZR Human angiostrongyliasis. Lancet Infect Dis. 2008;8:621–30.
- Cui Y, Shen M, Meng S. Lung CT Findings of angiostroglyliasis caused by Angiostrongylus cantonensis. Clinical Imaging. 2011;35:180-3.
- New D, Little MD, Cross J Angiostrongylus cantonensis infection from eating raw snails. N Engl J Med 1995;332:1105–6.
- Kliks MM, Palumbo NE. Eosinophilic meningitis beyond the Pacific Basin: the global dispersal of a peridomestic zoonosis caused by Angiostrongylus cantonensis, the nematode lungworm of rats. Soc Sci Med. 1992;34:199-212.
- Slom TJ, Cortese MM, Gerber SI,et al. An outbreak of eosinophilic meningitis caused by Angiostrongylus cantonensis in travelers returning from the Caribbean. N Engl J Med. 2002;346:668-675.
- Moreira VL, Giese EG, Melo FT, et al. Endemic angiostrongyliasis in the Brazilian Amazon: natural parasitism of Angiostrongylus cantonensis in Rattus rattus and R. norvegicus, and sympatric giant African land snails, Achatina fulica. Acta Trop. 2013;125(1):90-7
- Kim DY, Stewart TB, Bauer RW, Mitchell M. Parastrongylus (=Angiostrongylus) cantonensis now endemic in Louisiana wildlife. J Parasitol. 2002;88(5):1024.
- Campbell BG, Little MD. The finding of Angiostrongylus cantonensis in rats in New Orleans. Am J Trop Med Hyg. 1988;38:568-73.
- Chotmongkol V, Sawanyawisuth K, Thavornpitak Y. Corticosteroid treatment of eosinophilic meningitis. Clin Infect Dis. 2000;31:660–2.
- Jitpimolmard S, Sawanyawisuth K, Morakote N, et al. Albendazole therapy for eosinophilic meningitis caused by Angiostrongylus cantonensis. Parasitol Res. 2007;100:1293–6.
Home/Critical Care