
Correct!
2. Chest CT
Chest CT is the most appropriate step in the patient’s evaluation, given her respiratory complaints and abnormal chest radiographic findings. Bronchoscopy is also a reasonable choice, but she reportedly recently underwent this procedure, so it may be wise to attempt to obtain these results rather than repeat an invasive procedure. Thoracic MRA is primarily used for assessment of the large arteries of the thorax, which could prove useful given the reported history of central nervous system vasculitis, but there are few data to indicate the need for this procedure at this point. Surgical lung biopsy could prove useful given the chest radiographic findings, but these imaging findings are non-specific and are incompletely characterized at this point, and therefore surgical lung biopsy is premature. 18FDG-PET scan is clearly useful for the investigation of pulmonary abnormalities, typically in the context of staging suspected or known malignancies or for the assessment of indeterminate lung nodules, but is usually employed after characterization of pulmonary abnormalities with chest CT; therefore, 18FDG-PET scan is also premature at this juncture.
The patient’s bronchoscopy results reportedly showed possible Actinomyces israelii, and apparently, she was started on clindamycin (due to her penicillin allergy) and amphotericin to treat this presumed infection.
A chest CT performed during this hospitalization several months earlier (Figure 2) was located.
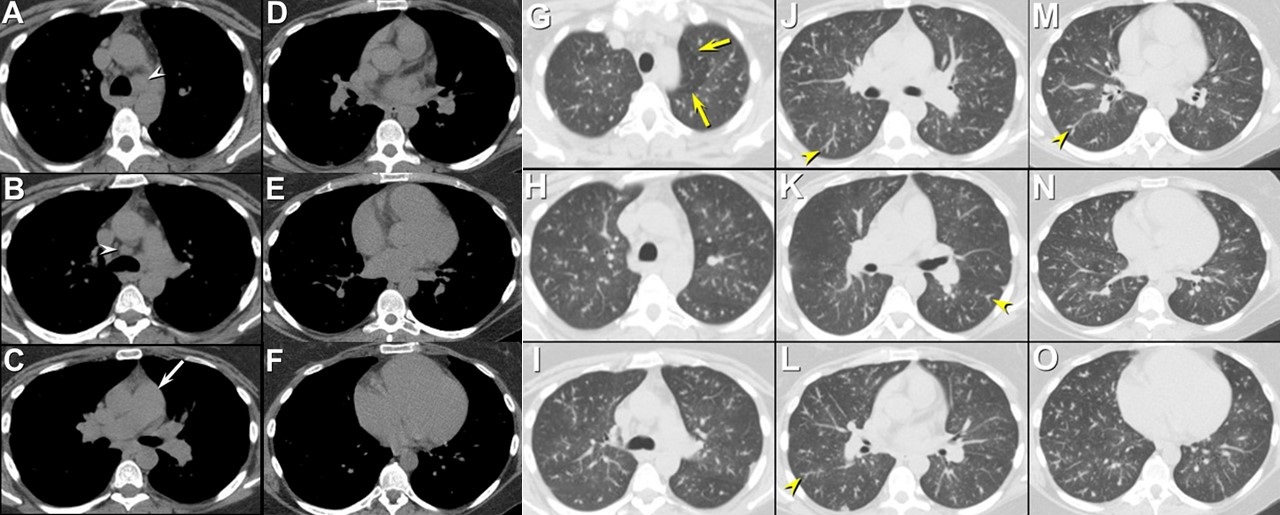

Figure 2. Representative static images from the axial unenhanced thoracic CT displayed in soft tissue windows (A-F) and in lung windows (G-O). Lower left: video of CT in soft tissue windows. Lower right: video of CT in lung windows.
Which of the following represents the most accurate assessment of the chest CT findings? (Click on the correct answer to proceed to the fourth of twelve pages)