
Correct!
4. 1 and 3
The patient has epiglottitis. Although the position of epiglottis is altered by the endotracheal tube, it is enlarged (Figure 2).
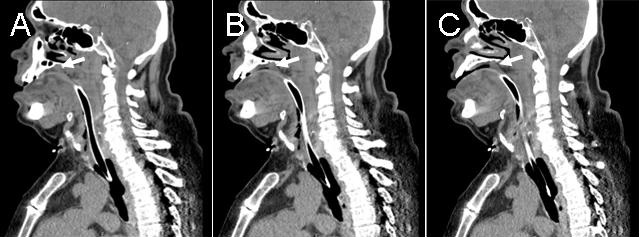
Figure 2. Neck CT scan showing enlarged epiglottis (arrows).
Many would confirm the presence of epiglottitis by direct laryngoscopy (Figure 3).
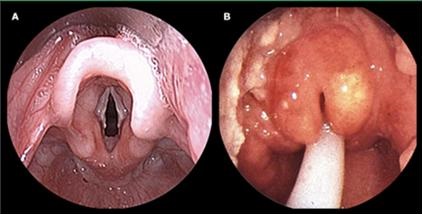
Figure 3. Direct laryngoscopy showing normal epiglottis on the left and an enlarged epiglottis on the right (not this patient) (1).
The epidemiology of epiglottis has changed since the introduction of Hemophilus influenza B vaccine in 1985. The incidence has decreased in children so that now epiglottitis is predominately an adult disease. While the majority of children presented with epiglottitis presented with difficulty breathing and stridor adults present somewhat differently (Table 1).
Table 1. Common symptoms in adults with epiglottitis.
The cause of the epiglottitis is infectious in most instances and antibiotics should to cover H. influenza, Streptococcus and Staphylococcus, the three most common bacterial causes. Many still give corticosteroids although trials in children have produced conflicting results (2-4). Many also give epinephrine (4).
Tracheostomy is not necessary in most cases. Most patients can be extubated after 48-72 hours if the epiglottic inflammation has been shown to decrease.
Our patient was given corticosteroids and vancomycin, ceftriaxone, and ampicillin/sulbactam. He was breathing comfortably on minimal ventilator settings when his urine output decreased to less than 100 ml/8 hours despite a Foley catheter in place which seemed to be functioning normally. Chest X-ray was unremarkable (Figure 4).

Figure 4. Portable chest radiograph on hospital day 2.
What should be done at this time? (Click on the correct answer to proceed to the fourth of six pages)