
Correct!
4. 1 and 3
There is opacification of the left chest on the radiograph. There is also volume loss on the left side. Note the deviation of the trachea to the left. A significant pleural effusion is unlikely with volume loss present.
The most likely cause of the volume loss in this patient’s situation is retained secretions in the left lung. The left lung is more difficult to suction than the right since the right mainstem bronchus is more in line with the trachea while the left mainstem bronchus is more at an angle making passage of the suction catheter into the left lung more difficult. Bronchoscopy was performed and copious amounts of secretions were removed from the left lung.
The patient was noted to have left-sided ptosis and decreased power 3/5 in his proximal upper and lower extremities. Reflexes were intact. Magnetic resonance imaging of the brain and brainstem were unremarkable. The possibility of diaphragmatic weakness was raised and ultrasound of the left diaphragm was performed (Figure 3).
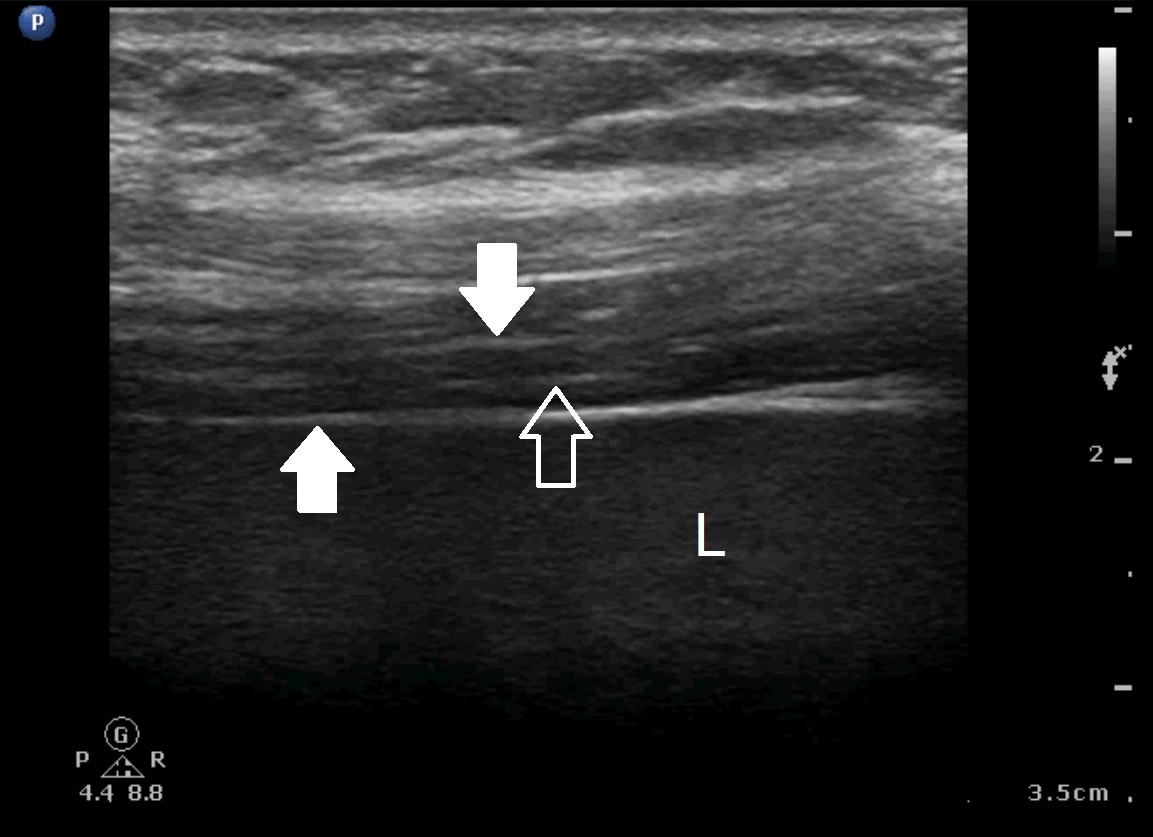
Figure 3. Left: Still image from diaphragmatic video. The echogenic edges of the diaphragm are labeled with solid white arrows, as is the characteristic central echogenic line (empty arrow) of the diaphragm. The liver is labelled with an “L”. Right: diaphramatic video.
Diaphragm thickening fraction (DTF) assessed by ultrasound was calculated using the following formula: Thickness at end inspiration - Thickness at end expiration / Thickness at end expiration. This patient’s DTF was found to 55%.
Which of the following are true? (Click on the correct answer to proceed to the fourth of six pages)