
Correct!
5. Tumor Thrombus
The echocardiogram shows a large solid echogenic mass in the right atrium. The mass seems to originate from the origin of the inferior vena cava / right atrial junction (Figure 3).
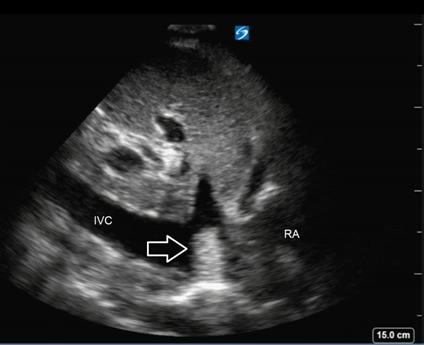
Figure 3. Still image of longitudinal inferior vena cava with arrow pointing to tumor thrombus and inferior vena cava (IVC) and right atrium (RA) labeled.
The right atrium is normal in size. There does not seem to be compromise the tricuspid valve. The right ventricle is normal in size and function. The left atrium and ventricle are also normal in size and function. The estimated ejection fraction is >70%. The imaging is most compatible with a tumor thrombus extending from the inferior vena cava. Myxomas normally originate from the intra-atrial septum or valve. Renal cell carcinoma and hepatocellular carcinoma are the most common tumors that spread to the heart via the inferior vena cava.
The patient was found to have esophageal varices requiring 12 bands by gastroenterology. Multiphase magnetic resonance imaging demonstrated a large arterially enhancing mass with smaller satellite lesions diagnostic of hepatocellular carcinoma. Additionally, there was direct extension of a large volume tumor thrombus into the right portal vein, which was also noted in the intrahepatic Inferior Vena Cava extending into the right atrium. The patient’s alpha- fetoprotein level was normal, consistent with non-secreting hepatocellular carcinoma.
Twenty five percent of cardiac masses are found to be atrial myxomas with the majority of masses being benign (1). This patient’s history of hepatitis C cirrhosis increased his risk of malignancy. At present, there is no expert consensus for management of tumor thrombus that is extending into the right atrium (2). Palliative resection may be necessary owing to hemodynamic compromise, but the prognosis remains very poor. In multiple case reports of tumor thrombus resection, there was no improvement in survival or outcomes (3,4). At this time, it is uncertain that resection of tumor thrombus will yield any additional benefit to our patient.
References