
Correct!
4. 1 and 3
The patient almost certainly has lung cancer. The volume loss in the right upper lobe suggests endobronchial obstruction. A needle biopsy would likely yield a diagnosis and is not wrong, but most would prefer bronchoscopy with a suspected endobronchial obstruction (1). Needle biopsy has a higher complication rate, and enlarged mediastinal lymph nodes can be sampled during bronchoscopy (1).
The patient underwent a chest PET/CT scan which the mass along with enlarged mediastinal lymph nodes with accumulation of radioactive glucose indicating probable metastatic disease. Bronchoscopy showed a right upper lobe endobronchial mass which on biopsy was a non-small cell cancer of the lung TTP-1 positive. He was begun on etoposide and cisplatin with radiation.
He subsequently developed a large right pleural effusion. An attempt was made to insert an indwelling PleurX catheter for drainage but this was unsuccessful. In November, 2015 pemetrexed and carboplatin was recommended with a plan for 2 cycles and a restaging evaluation. He took dexamethasone in preparation but developed night sweats, cough, increasing shortness of breath, upper respiratory symptoms and a productive cough.
A chest radiograph was performed (Figure 2).
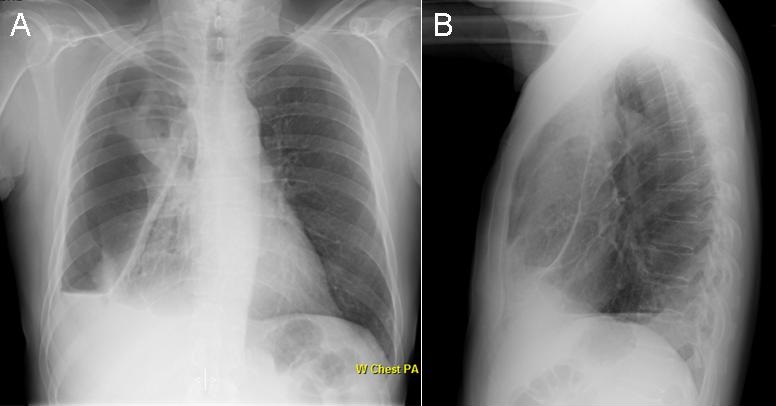
Figure 2. Chest radiograph.
Which of the following are true regarding the chest radiograph? (Click on the correct answer to proceed to the fourth of five panels)