Phoenix Pulmonary and Critical Research and Education Foundation
Gilbert, AZ
History of Present Illness
You are asked to see a 35-year-old man who was admitted to the ICU from the ER the previous night with an exacerbation of his chronic obstructive pulmonary disease (COPD). He has a long history of COPD and came to the ER for COVID-19 testing because he was at a party where a friend was later found to COVID-19. He denies any change in his chronic respiratory symptoms but his spirometry was significantly worse than his baseline in the ER and despite his protests he was admitted. He was treated with empiric antibiotics (amoxicillin and clavulanic acid), corticosteroids (methylprednisolone 125 mg every 6 hours), bronchodilators (albuterol/ipratropium every 4 hours) and oxygen. He says his breathing has not improved and he wants to go home. He has had gradually increasing shortness of breath for the past 8-10 years. He has minimal cough but denied any fevers, systemic symptoms, or wheezing.
PMH, FH, and SH
He had a history of multiple pneumothoraces which eventually led to bilateral pleurodesis. He has had not pneumothoraces since. He had a benign bone tumor removed about 25 years ago and a history of manic-depression. There is no FH of any similar type of problems. He does smoke about 3/4 pack of cigarettes per day and has more than occasional marijuana use.
Physical Exam
Physical examination was unremarkable expect for a well-healed scar on the left thigh.
Spirometry
Previous spirometry performed as an outpatient showed his FVC 2.54 L (53% of predicted) with an FEV1 1.25 L (31% of predicted). These improved to 2.99 L and 1.52 L after a bronchodilator. His spirometry last night in the ER was FVC 1.63 L (29 % predicted) and FEV1 0.80 L (18 % predicted).
Radiography
A chest radiograph was performed (Figure 1).
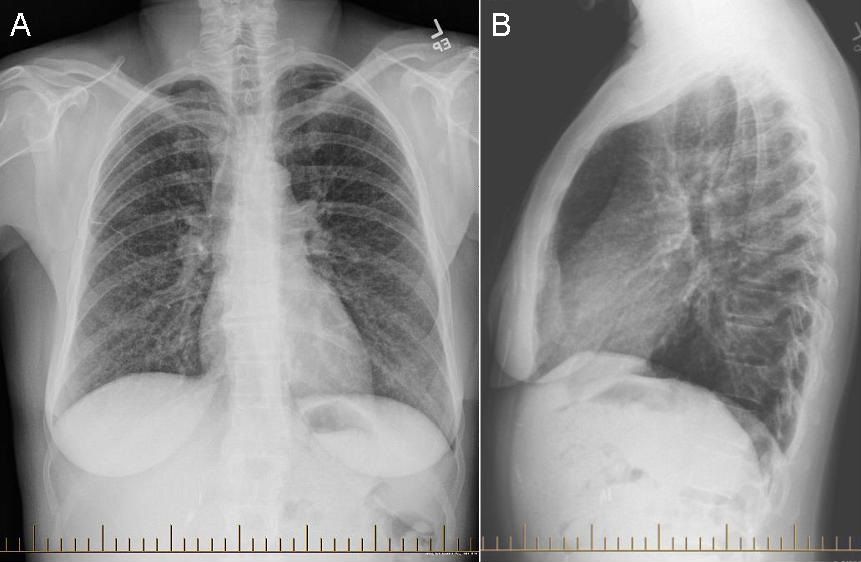 Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
What should be done at this time? (Click on the correct answer to be directed to the second of five pages)
- Continue his antibiotics, corticosteroids and bronchodilators
- Order an alpha-1 antitrypsin level
- Transfer to the floor
- 1 and 3
- All of the above