
Alveolopleural Fistula In COVID-19 Treated with Bronchoscopic Occlusion with a Swan-Ganz Catheter
Nathaniel Hitt DO1
Aleksey Tagintsev DO1
Douglas Summerfield MD1
Evan Schmitz MD2
1MercyOne North Iowa Medical Center, Des Moines, IA USA
2Airod Medical, Gainesville, FL USA
Abstract
Pneumothorax and pneumomediastinum are known complications of COVID-19 patients. They have been documented to occur both with and without mechanical ventilation. There are several reports of cases further complicated by alveolopleural or bronchopleural fistulas. However, there are no studies and only a few case reports on the treatment options used for alveolopleural fistulas in COVID-19 patients. To our knowledge, there is only one report of bronchoscopic treatment with endobronchial valves in a COVID-19 patient. We present the case of a 63-year-old male with COVID-19, pneumothorax, and an alveolopleural fistula that was successfully sealed using bronchoscopic occlusion with a Swan-Ganz catheter.
Abbreviation List
- COVID-19: Severe acute respiratory distress syndrome coronavirus-2
- PAL: Persistent air leak
- APF: Alveolopleural fistula
- PaO2: Partial pressure of arterial oxygen
- FiO2: Fraction of inspired oxygen
Background
Pneumothorax complicates 1% of COVID-19 hospital admissions and the risk increases with mechanical ventilation (1). There have been several reports of pneumothoraces in COVID-19 complicated by persistent air leaks (PAL) and alveolopleural fistulas (APFs) (1-3). APFs are a communication between the pulmonary parenchyma of the alveoli and the pleural cavity. The most common cause is lung reduction surgery, but it can also be present following spontaneous pneumothorax. Less commonly it can be caused by pulmonary infection. Clinically, APFs present as a PAL on chest tube drainage with a PAL defined as a duration greater than 5 days. Complications include pleural infection and ventilation/perfusion mismatch with a loss of positive end expiratory pressure. APFs in non-COVID patients have been associated with an increased duration of chest tube, prolonged hospital stay, and increased morbidity a drainage and mortality. Treatments in non-COVID patients have ranged from insertion of additional thoracostomy tubes, surgical intervention, and bronchoscopic intervention (2). There is one reported case of an APF in COVID-19 successfully treated with endobronchial valves (3). Here we present the case of an APF in COVID-19 treated with bronchoscopic occlusion with a Swan-Ganz catheter.
Case Presentation
The patient was a 63-year-old man diagnosed with COVID-19 who required intubation, mechanical ventilation, and admission to the critical care unit. On hospital day 2 chest x-ray revealed bilateral pneumothoraces requiring chest tube placement. Bilateral PAL was present and on hospital day 10 the patient developed a moderate sized right sided pneumothorax despite the adequately positioned chest tube. The initial thoracostomy tube was replaced with a large bore chest tube with immediate resolution of the pneumothorax. However, a moderate air leak persisted and by hospital day 14, the diagnosis of APF was suspected. Bronchoscopic occlusion using the balloon of a Swan-Ganz catheter was performed.
A Swan-Ganz catheter was inserted through the endotracheal tube and along-side of a bronchoscope. The balloon was sequentially inflated and deflated to occlude each lobe to assess for air leak resolution. The air leak was reduced, but not resolved with occlusion of the right lower lobe and right middle lobe individually. The balloon was inflated just enough to occlude the right bronchus intermedius with near complete resolution of the leak (Figure 1).
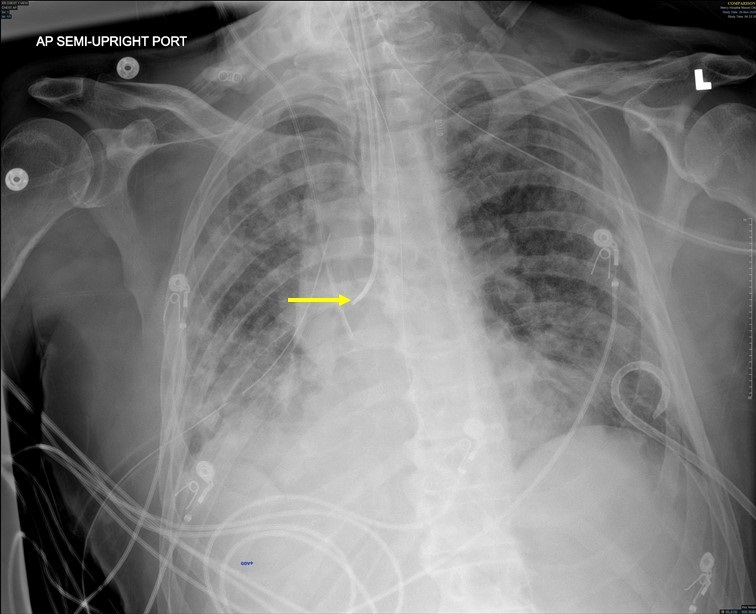
Figure 1. Chest radiograph showing Swan-Ganz catheter (yellow arrow) with its cuff inflated in the right bronchus intermedius to seal an alveolopleural fistula.
The patient was observed for ten minutes to ensure tolerability before concluding the procedure. He was kept paralyzed to reduce coughing. After 3 days the air leak resolved, the Swan-Ganz catheter was removed, and the air leak remained sealed. The PaO2:FiO2 ratio improved from 79 to 250. However, despite initial improvement and no air leak the patient's conditioned worsened in the setting of multisystem organ failure. Multisystem organ failure was attributed to a combination of severe acute respiratory distress syndrome, cytokine storm, and septic shock from a urinary tract infection. The patient's family made the decision to withdraw care on day 22.
Discussion
Despite several cases of refractory pneumothorax in COVID-19, the significance and optimal treatment remains unclear (1,3,4). There is one report of two COVID-19 patients treated with thoracoscopy, bleb resection, and pleurectomy(4) and a single report of endobronchial valves (3). Conservative management with prolonged chest tube remains the recommended treatment (2). The American College of Chest Physicians guidelines only recommend bronchoscopic treatment in refractory cases when surgery is not possible (2). This patient was not a surgical candidate due to his instability, endobronchial valves were unavailable at our facility, and at height of the COVID-19 pandemic, transfer to a tertiary care center was not possible. Bronchoscopic occlusion with a balloon catheter has been described previously in a case a of PAL secondary to polymicrobial pneumonia, pulmonary interstitial emphysema, and in a case of necrotic lung complicated by hydropneumothorax (2,5,6). Bronchoscopy in COVID-19 is associated with an increased risk of infection and its use should be limited if possible. In this case, it was determined that with proper personal protective equipment and lack of access to other treatments, bronchoscopic occlusion was the best option.
An 8.0 French Swan-Ganz catheter was selected for its balloon that connects to an integrated stopcock to maintain inflation and for its relative availability. We classified the PAL as an APF after the leak was revealed to be distal to the segmental bronchi. The average time to resolution is reported to be 4-7.5 days (2). The decision to maintain occlusion for 3 days was based on the above average, patient improvement, and the lack of drainage from the occluded lung. The risk of infection, in particular pneumonia and empyema, must be considered when using this technique. Ideally, an endobronchial valve would have been available to allow a one-way valve to drain secretions (2). Our patient was closely monitored for developing pulmonary infection with daily chest radiography and, following the removal of the Swan-Ganz Catheter, a bacterial sputum culture which was negative.
Conclusion
There are no randomized controlled trials investigating which treatment of PALs is most effective or safe in COVID-19 patients or even in non-COVID-19 patients (2). Furthermore, pneumothorax and persistent air leaks in COVID-19 patients have not been universally shown to increase mortality (1). However, considering the known morbidity and mortality associated with PALs, we suggest it may be reasonable in cases refractory to thoracostomy tube to treat with a Swan-Ganz catheter when otherresources are not available.
Acknowledgement
Peter L. Larsen PhD for editorial and administrative support.
References
- Martinelli AW, Ingle T, Newman J, et al. COVID-19 and pneumothorax: a multicentre retrospective case series. Eur Respir J. 2020 Nov 19;56(5):2002697. [CrossRef] [PubMed]
- Sakata KK, Reisenauer JS, Kern RM, Mullon JJ. Persistent air leak - review. Respir Med. 2018 Apr;137:213-218. [CrossRef] [PubMed]
- Pathak V, Waite J, Chalise SN. Use of endobronchial valve to treat COVID-19 adult respiratory distress syndrome-related alveolopleural fistula. Lung India. 2021 Mar;38(Supplement):S69-S71. [CrossRef] [PubMed]
- Aiolfi A, Biraghi T, Montisci A, et al. Management of Persistent Pneumothorax With Thoracoscopy and Bleb Resection in COVID-19 Patients. Ann Thorac Surg. 2020 Nov;110(5):e413-e415. [CrossRef] [PubMed]
- Ellis JH, Sequeira FW, Weber TR, Eigen H, Fitzgerald JF. Balloon catheter occlusion of bronchopleural fistulae. AJR Am J Roentgenol. 1982 Jan;138(1):157-9. [CrossRef] [PubMed]
- Schmitz ED. A new interventional bronchoscopy technique for the treatment of bronchopleural fistula. Southwest J Pulm Crit Care. 2017;15(4):174-8. [CrossRef]
Cite as: Hitt N, Tagintsev A, Summerfield D, Schmitz E. Alveolopleural Fistula In COVID-19 Treated with Bronchoscopic Occlusion with a Swan-Ganz Catheter. Southwest J Pulm Crit Care. 2021;23(4):100-3. doi: https://doi.org/10.13175/swjpcc026-21 PDF
 Post a Comment
Post a Comment
Reader Comments