
Correct!
2. A normal pCO2 excludes hypoventilation as a cause of hypoxemia
There are five causes of hypoxemia (1).
- Ventilation-perfusion mismatching is the most common cause and occurs when blood passes through non- or poorly ventilated alveoli. Diseases such as pulmonary embolism can also be associated with hypoxemia but the cause is not the lack of perfusion but the release of mediators by the clot which cause ventilation-perfusion mismatching in other areas of the lung.
- Hypoventilation results when a lack of alveolar ventilation causes results in an increased PaCO2 and a decreased oxygen tension in the blood. In the postoperative setting this is most commonly due to excessive administration of narcotics for pain.
- Low inspired FiO2 can cause hypoxemia but reversing the lines on the ventilator is virtually impossible because the oxygen and air connections differ.
- Alveolar-capillary block occurs when there is insufficient time for the blood passing through a capillary to become fully saturated before returning to the left side of the heart. This is due to thickening between the capillary and alveolus because of collage formation. Most hemoglobin is fully saturated after one-tenth of its passage through the capillary and this reserve makes this unlikely at rest. Alveolar-capillary block only becomes a clinical factor with a marked reduction in transit time mostly commonly due to exercise.
- A right-to-left shunt in the heart or lung results in non-oxygenated blood passing to the arterial circulation. Many of the causes are congenital but can present in adulthood.
The patient had an arterial blood gas with a PaO2 of 49 mm Hg, a PaCO2 of 35, and a pH of 7.35 on ventilator settings of a FiO2 of 100%, SIMV 12 breaths/min, tidal volume of 600 ml, pressure support of 14 cm H2O, and peep of 8 cm H2O.
A chest x-ray was taken (Figure 1).
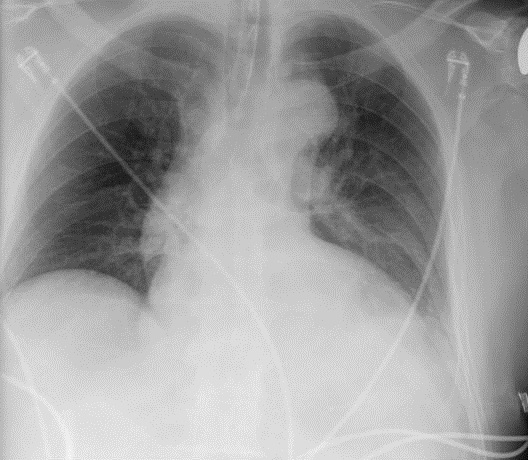
Figure 1. Post-operative portable chest x-ray.
Which of the following is true?
- A normal chest x-ray in a hospitalized hypoxic patient should prompt a search for a pulmonary embolism.
- The endotracheal tube is misplaced which is the likely cause of the hypoxemia.
- The chest x-ray shows left lower lung atelectasis and/or pleural effusion which likely explain the hypoxemia.
- The chest x-ray shows pulmonary edema.
- The chest x-ray shows bilaterally paralyzed diaphragms.
Home/Critical Care