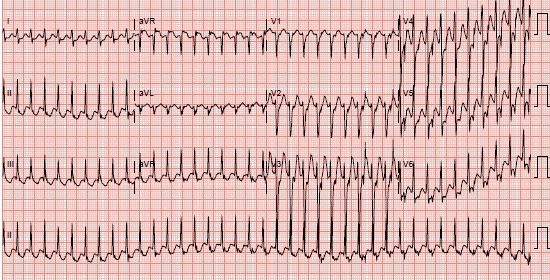
Figure 1. Presenting EKG with supraventricular tachycardia at rate of 232.
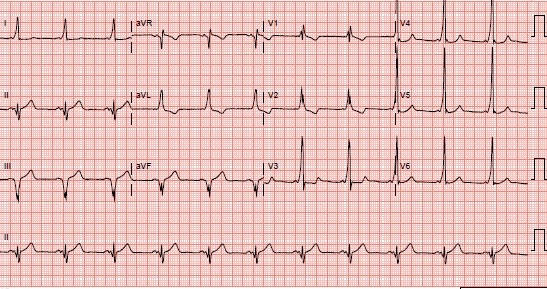
Figure 2. Post-conversion EKG demonstrating a short PR interval, slurring of the initial QRS upslope (delta wave), widened QRS, and ST-T repolarization change; characteristic of Wolff-Parkinson-White Syndrome.
A 38-year-old man developed sustained rapid heart rate while rock climbing. The patient reported that he had experienced rare bouts of self-limited palpitations in the past. Blood pressure on arrival to the emergency department was 112/ 65 mm Hg. The patient’s initial EKG demonstrated a regular, narrow complex supraventricular tachycardia, with a rate of 232 (Figure 1). Intravenous adenosine was administered with no change in his rate or rhythm. The patient then received amiodarone by intravenous bolus, with subsequent conversion to sinus rhythm (Figure 2).
Wolff-Parkinson-White (WPW) syndrome is a congenital cardiac condition present in approximately 0.15% of the general population. WPW is characterized by the abnormal presence of conduction tissue that creates an accessory atrioventricular pathway and thus potentiates reentrant tachycardia (1). The classic resting EKG findings in WPW are: a shortened PR interval (less than 0.12 seconds), an indistinct initial upslope of the QRS complex (known as the delta wave), a widened QRS complex (0.12 seconds or greater), and ST-T repolarization changes (2). In WPW presenting as a narrow complex tachycardia without hypotension, the initial treatment is adenosine or a calcium channel blocker, followed by amiodarone if unsuccessful. If the presenting rhythm is atrial fibrillation, atrial flutter, or an undefined wide complex tachycardia without hypotension, amiodarone is used. A hemodynamically unstable rhythm warrants immediate electrical cardioversion. Definitive evaluation and treatment of WPW requires electrophysiologic mapping and subsequent ablation of the accessory pathway.
Charles Van Hook MD, Cristina Demian MD, Douglas Tangel MD, Jennifer Blair MD, and Lisa Patel MD
Avista Adventist Hospital
Louisville, Colorado USA
References
- Katritsis DG, Camm AJ. Atrioventricular nodal reentrant tachycardia. Circulation. 2010 Aug 24;122(8):831-40. [CrossRef] [PubMed]
- Mark DG, Brady WJ, Pines JM. Preexcitation syndromes: diagnostic consideration in the ED. Am J Emerg Med. 2009 Sep;27(7):878-88. [CrossRef] [PubMed]
- Khairy P, Van Hare GF, Balaji S, et al. PACES/HRS expert consensus statement on the recognition and management of arrhythmias in adult congenital heart disease. Heart Rhythm. 2014 Oct;11(10):e102-65. [CrossRef] [PubMed]
Cite as: Van Hook C, Demian C, Tangel D, Blair J, Patel L. Medical image of the week: Wolff-Parkinson-White syndrome. Southwest J Pulm Crit Care. 2017;14(4):164-5. doi: https://doi.org/10.13175/swjpcc046-17 PDF