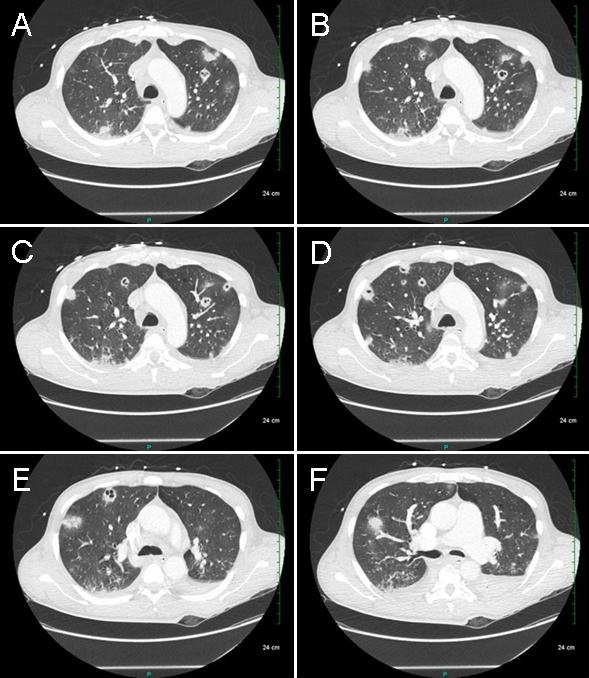
Figure 1. Panels A-F: Selected static images from the thoracic CT showing numerous septic pulmonary emboli with cavitation. Lower panel: movie of selected images from thoracic CT scan.
A 46-year-old man was admitted with altered mental status. His past medical history included HIV/AIDS on HAART therapy, hepatitis B and C, non-Hodgkin's lymphoma (NHL), deep venous thrombosis with insertion of an inferior vena caval filter, and poly-substance abuse. Vitals revealed fever and tachycardia. On exam, he was lethargic and confused, and had bilateral crackles on lung auscultation. Computerized axial tomography (CT) of the head was unremarkable and chest X-ray revealed patchy nodular infiltrates in the right upper lobe and bilateral lower lobes. Work up for an infectious cause was initiated including opportunistic infections and he was started on empiric antibiotics for pneumonia. On Day 2, his roommate who came to visit him, revealed that he was recently admitted in another hospital for headache and flu-like symptoms, and discharged with a peripherally inserted central catheter (PICC) in place as he was scheduled for a positron emission tomography (PET) the next morning for evaluation of recurrence of NHL. However, he presented for the PET scan 10 days after discharge, during which period he was abusing heroin through the PICC line. A thoracic CT was also obtained which showed innumerable scattered cavitary pulmonary opacities with peripheral ground glass opacities consistent with septic pulmonary emboli in the right and left upper lobe and right middle lobe (Figure 1). Blood and urine cultures grew methicillin-resistant Staphylococcus aureus, CD4 count was 180, cryptococcus and histoplasma antigens were negative, as were urine antigens for pneumococcus and legionella. He was also found to have deep venous thrombosis of the right upper extremity. Trans-esophageal echocardiogram was negative for valvular vegetations. He was successfully treated with vancomycin and rifampin and discharged home.
Septic pulmonary emboli are embolization of infectious particles into the lungs via the pulmonary arterial system. Septic pulmonary emboli can occur from varying sources. Patients may be asymptomatic or present with sepsis. CXR shows multiple nodules in the periphery of the lower lobes. CT chest may show feeding vessel sign (a vessel coursing directly to a nodule or mass) in 50% of patients. Early diagnosis and prompt treatment can lead to a successful outcome.
Nanditha Malakkla MD and Chandramohan Meenakshisundaram MD
St. Francis Hospital
Evanston, IL
References
- Fidan F, Acar M, Unlu M, Cetinkaya Z, Haktanir A, Sezer M. Septic pulmonary emboli following infection of peripheral intravenous cannula. Eur J Gen Med. 2006;3:132–5.
- Kuhlman JE, Fishman EK, Teigen C. Pulmonary septic emboli: Diagnosis with CT. Radiology. 1990;174:211–3. [CrossRef] [PubMed]
- Hind CR. Pulmonary complications of intravenous drug misuse. 1. Epidemiology and non-infective complications. Thorax 1990; 45:891-8. [CrossRef] [PubMed]
Reference as: Malakkla N, Meenakshisundaram C. Medical image of the week: septic emboli. Southwest J Pulm Crit Care. 2014;9(3):183-4. doi: http://dx.doi.org/10.13175/swjpcc120-14 PDF